
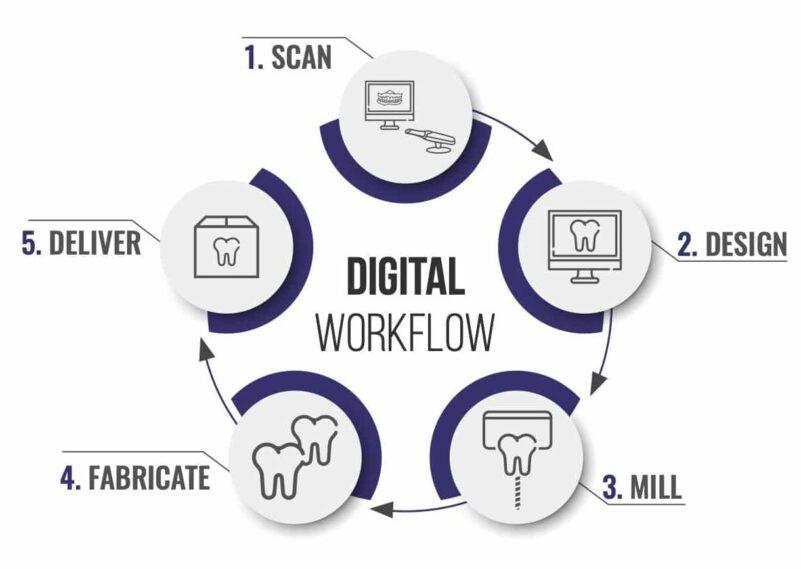
In digital dental workflows, CAD design is often perceived as a standardized service—one that can be evaluated primarily by speed or cost. However, from a laboratory perspective, this assumption does not hold under real production conditions. The variability in dental CAD design quality becomes evident when cases move beyond initial design into manufacturing, fitting, and clinical delivery.
The distinction between low-cost CAD design and lab-grade precision is not defined by software alone. Both may use similar tools. The difference lies in how workflows are structured, how input data is validated, how design decisions are controlled, and how consistently results are delivered across varying case conditions.
This article examines the operational differences between low-cost and lab-grade CAD design, focusing on workflow stability, risk exposure, and long-term efficiency.
Low-cost CAD services are often positioned around reduced pricing or faster turnaround. However, cost is not an isolated variable—it reflects how the workflow is structured.
These characteristics allow for lower operational cost per case but introduce variability into the workflow.
In this context, dental CAD design quality is not a feature—it is the result of process discipline.
The most immediate difference between low-cost and lab-grade design appears at the intake stage.
When intake is not controlled:
Lab-grade workflows prioritize input quality to stabilize the entire process.
Design decisions may rely on default parameters rather than case-specific considerations.
This approach ensures that dental CAD design quality is consistent across cases, not dependent on individual interpretation.
Margin definition is one of the most sensitive aspects of CAD design.
Poor margin handling leads to:
These outcomes directly affect workflow efficiency beyond the design stage.
Occlusion is another area where differences in dental CAD design quality become evident.
Inaccurate occlusion leads to:
Lab-grade design reduces these issues by integrating occlusal considerations into the workflow.
A critical distinction between low-cost and lab-grade CAD design lies in how well designs translate into production.
This alignment ensures that design intent is preserved through fabrication.
This multi-layered QC structure reduces cumulative error and improves overall dental CAD design quality.
Communication is often reduced in low-cost workflows to maintain speed.
Clear communication reduces:
Low-cost services often emphasize faster turnaround. However, speed must be evaluated across the full workflow.
Low-cost workflows may introduce:
These factors extend total case time, even if initial design appears faster.
Scalability is a key consideration in dental CAD design quality.
Consistency becomes more critical as case volume increases.
Selecting low-cost CAD design introduces specific operational risks.
Lab-grade design reduces these risks by prioritizing process control over short-term efficiency.
Low-cost models may be appropriate in specific scenarios:
However, even in these cases, workflow impact should be considered.
Lab-grade dental CAD design quality is essential for:
In these contexts, consistency and predictability outweigh initial cost considerations.
A practical evaluation framework includes:
This framework shifts the focus from cost to system performance.
The difference between low-cost CAD design and lab-grade precision is not defined by tools or individual skills. It is defined by how the workflow is structured and controlled.
Dental CAD design quality determines not only the accuracy of individual restorations but also the efficiency and stability of the entire production process. While low-cost options may offer short-term advantages, they often introduce variability that affects long-term outcomes.
From a laboratory perspective, selecting a design model is not a pricing decision—it is a workflow decision that influences every stage from intake to final delivery.
The distinction between low-cost CAD design and lab-grade precision is not defined by software alone. Both may use similar tools. The difference lies in how workflows are structured, how input data is validated, how design decisions are controlled, and how consistently results are delivered across varying case conditions.
This article examines the operational differences between low-cost and lab-grade CAD design, focusing on workflow stability, risk exposure, and long-term efficiency.
Cost as an Output of Process, Not a Primary Variable
Low-cost CAD services are often positioned around reduced pricing or faster turnaround. However, cost is not an isolated variable—it reflects how the workflow is structured.
Characteristics of Cost-Driven Models
- Minimal intake validation
- High throughput with limited case segmentation
- Reduced time allocated per case
- Limited communication or feedback loops
These characteristics allow for lower operational cost per case but introduce variability into the workflow.
Characteristics of Lab-Grade Models
- Structured intake quality control
- Defined design protocols
- Integrated quality assurance
- Consistent communication processes
In this context, dental CAD design quality is not a feature—it is the result of process discipline.
Intake Discipline: The First Point of Divergence
The most immediate difference between low-cost and lab-grade design appears at the intake stage.
Low-Cost Intake Approach
- Cases are accepted with minimal validation
- Missing or unclear data is often handled during design
- Designers may proceed with assumptions to maintain speed
Lab-Grade Intake Approach
- Cases are reviewed for completeness before design begins
- Required scan sets and parameters are verified
- Incomplete cases are paused until clarified
Workflow Impact
When intake is not controlled:
- Design workflows are interrupted
- Errors propagate downstream
- Turnaround time becomes inconsistent
Lab-grade workflows prioritize input quality to stabilize the entire process.
Design Execution: Throughput vs Controlled Precision
Low-Cost Design Characteristics
- Emphasis on speed and volume
- Limited time per case
- Reduced customization based on clinical context
Design decisions may rely on default parameters rather than case-specific considerations.
Lab-Grade Design Characteristics
- Structured application of design protocols
- Consideration of margin integrity, occlusion, and material constraints
- Alignment with manufacturing requirements
This approach ensures that dental CAD design quality is consistent across cases, not dependent on individual interpretation.
Margin Handling and Its Downstream Consequences
Margin definition is one of the most sensitive aspects of CAD design.
In Low-Cost Workflows
- Margins may be approximated when scan data is unclear
- Limited time is spent refining margin lines
- Variability increases across cases
In Lab-Grade Workflows
- Margin clarity is validated at intake
- Designers refine margins based on clear data
- Consistency is maintained across restorations
Impact on Fit and Remakes
Poor margin handling leads to:
- Open or overextended margins
- Increased chairside adjustment
- Higher remake rates
These outcomes directly affect workflow efficiency beyond the design stage.
Occlusal Design: Simplification vs Controlled Adjustment
Occlusion is another area where differences in dental CAD design quality become evident.
Low-Cost Approach
- Simplified occlusal mapping
- Reduced emphasis on contact distribution
- Greater reliance on default articulation settings
Lab-Grade Approach
- Controlled occlusal contact design
- Consideration of load distribution
- Alignment with clinical input and case requirements
Workflow Implications
Inaccurate occlusion leads to:
- Chairside adjustments
- Patient discomfort
- Additional clinical time
Lab-grade design reduces these issues by integrating occlusal considerations into the workflow.
Design-to-Manufacturing Alignment
A critical distinction between low-cost and lab-grade CAD design lies in how well designs translate into production.
Low-Cost Limitations
- Designs may not fully account for material constraints
- Thickness and connector parameters may be inconsistent
- Production adjustments may be required
Lab-Grade Integration
- Design parameters are aligned with manufacturing capabilities
- Material-specific constraints are considered
- Output is consistent with production requirements
This alignment ensures that design intent is preserved through fabrication.
Quality Control: Reactive vs Embedded Systems
Low-Cost QC Approach
- Limited or final-stage inspection
- Issues identified after design completion
- Corrections handled reactively
Lab-Grade QC Approach
- Intake-level validation
- Design-level review
- Pre-production verification
This multi-layered QC structure reduces cumulative error and improves overall dental CAD design quality.
Communication Structure and Case Clarity
Communication is often reduced in low-cost workflows to maintain speed.
Low-Cost Communication
- Minimal clarification during intake
- Limited feedback to clinics
- Reduced documentation of case details
Lab-Grade Communication
- Structured case submission requirements
- Clear documentation of design parameters
- Feedback loops for improving input quality
Workflow Impact
Clear communication reduces:
- Misinterpretation of cases
- Design variability
- Delays caused by clarification
Turnaround Time: Perceived Speed vs Actual Efficiency
Low-cost services often emphasize faster turnaround. However, speed must be evaluated across the full workflow.
Immediate Processing vs Stable Flow
- Low-cost: faster initial processing, higher risk of rework
- Lab-grade: controlled intake, consistent processing timelines
Hidden Delays
Low-cost workflows may introduce:
- Additional communication during design
- Remakes due to inaccuracies
- Production adjustments
These factors extend total case time, even if initial design appears faster.
Consistency Across Case Volume
Scalability is a key consideration in dental CAD design quality.
Low-Cost Scalability
- High volume capacity
- Increased variability under load
- Reduced consistency across cases
Lab-Grade Scalability
- Structured workflows maintain consistency
- Capacity is managed without compromising quality
- Output remains stable across varying volumes
Consistency becomes more critical as case volume increases.
Risk Distribution in Design Choices
Selecting low-cost CAD design introduces specific operational risks.
Short-Term Benefits
- Lower cost per case
- Faster initial turnaround
Long-Term Risks
- Increased remake rates
- Higher chairside adjustment time
- Workflow instability
Lab-grade design reduces these risks by prioritizing process control over short-term efficiency.
When Low-Cost CAD Design May Be Suitable
Low-cost models may be appropriate in specific scenarios:
- Non-critical or temporary restorations
- Cases with low complexity
- Situations where variability can be tolerated
However, even in these cases, workflow impact should be considered.
When Lab-Grade Precision Becomes Critical
Lab-grade dental CAD design quality is essential for:
- Implant restorations
- Multi-unit bridges
- Full-arch cases
- High-volume production environments
In these contexts, consistency and predictability outweigh initial cost considerations.
Evaluating CAD Design Quality Beyond Cost
A practical evaluation framework includes:
Input Handling
- Does the provider validate case data before design?
Design Consistency
- Are results repeatable across cases?
Workflow Integration
- Is design aligned with manufacturing requirements?
Communication Structure
- Are case instructions clearly defined and documented?
This framework shifts the focus from cost to system performance.
Conclusion: Design Quality as a Workflow Decision
The difference between low-cost CAD design and lab-grade precision is not defined by tools or individual skills. It is defined by how the workflow is structured and controlled.
Dental CAD design quality determines not only the accuracy of individual restorations but also the efficiency and stability of the entire production process. While low-cost options may offer short-term advantages, they often introduce variability that affects long-term outcomes.
From a laboratory perspective, selecting a design model is not a pricing decision—it is a workflow decision that influences every stage from intake to final delivery.
Selecting an outsourcing partner is no longer a peripheral decision in digital dentistry. As workflows become increasingly dependent on CAD design, digital case intake, and integrated production systems, the performance of an external laboratory directly affects clinical timelines, restoration accuracy, and operational stability.
Dental outsourcing lab selection should not be based on isolated factors such as speed or cost. From a laboratory perspective, reliability is defined by how consistently a partner maintains workflow continuity—across intake, design, production, and communication—under varying case conditions.
This article outlines a structured framework for evaluating outsourcing laboratories, focusing on three core dimensions: quality control discipline, communication structure, and consistency in execution.
A common misconception is that reliability is determined by technical skill alone. In practice, most laboratories can produce acceptable results under controlled conditions. The difference emerges when:
A reliable partner maintains stable performance under these conditions. This requires not only technical capability but also structured processes that govern how cases are handled at every stage.
In dental outsourcing lab selection, the focus should shift from individual outputs to system behavior.
The intake stage is the earliest point at which workflow stability can be assessed.
A structured intake process includes:
Cases that do not meet these criteria are not processed immediately. Instead, they are paused until sufficient information is provided.
Labs that bypass intake validation may appear faster initially but introduce downstream inefficiencies:
A reliable laboratory enforces intake QC consistently, even if it delays individual cases. This approach stabilizes the overall workflow.
Communication is often underestimated in outsourcing relationships. However, it is one of the primary determinants of workflow efficiency.
Reliable laboratories define:
These elements ensure that dental outsourcing lab selection is not dependent on informal or ad hoc communication.
When communication is structured:
Conversely, unstructured communication leads to fragmented workflows and unpredictable turnaround times.
Consistency in CAD design is a key indicator of reliability. It reflects how well a laboratory standardizes its internal processes.
Consistency reduces variability, which is essential for maintaining efficiency at scale.
When design approaches vary:
In dental outsourcing lab selection, consistency is often more valuable than peak performance on individual cases.
A reliable outsourcing laboratory does not treat design and production as separate functions. Instead, it ensures that both stages are aligned.
Design must account for:
If design decisions are not aligned with manufacturing capabilities, issues arise during fabrication.
When design and production are coordinated:
This integration is a critical factor in evaluating outsourcing partners.
Turnaround time is often used as a primary selection criterion. However, its significance lies in consistency rather than speed.
Turnaround time should reflect a controlled process rather than reactive execution.
Reliable laboratories structure their timelines based on:
For example, design timelines are typically adjusted based on case size and complexity rather than applied uniformly.
Transparency in workflow management is another key indicator of reliability.
These systems allow both laboratory and clinic to monitor progress without relying on manual follow-up.
Transparency supports accountability and enhances overall efficiency.
In real-world workflows, variability is unavoidable. Reliable laboratories are defined by how they manage it.
Reliable partners implement:
This ensures that variability does not translate into workflow instability.
As case volume increases, the ability to scale becomes critical.
In dental outsourcing lab selection, scalability determines whether a partner can support long-term growth.
Quality control is often associated with final inspection. In reliable workflows, it is distributed across multiple stages.
This layered approach reduces cumulative error and improves overall accuracy.
Quality control, when applied consistently, becomes a driver of efficiency rather than a constraint.
Selecting a laboratory also involves assessing operational risk.
Reliable laboratories reduce risk by:
This structured approach supports long-term collaboration.
Based on workflow considerations, a reliable laboratory can be evaluated across three core dimensions:
This framework shifts the focus from isolated capabilities to system-level performance.
Dental outsourcing lab selection is fundamentally a decision about workflow structure. A reliable laboratory is not defined by individual strengths but by its ability to maintain consistent performance across all stages of the process.
From intake validation and communication to design consistency and production alignment, each element contributes to overall reliability. Laboratories that enforce structured workflows, maintain transparency, and manage variability effectively provide a more stable foundation for long-term collaboration.
In digital dental workflows, reliability is not an outcome—it is a property of the system that produces it.
Dental outsourcing lab selection should not be based on isolated factors such as speed or cost. From a laboratory perspective, reliability is defined by how consistently a partner maintains workflow continuity—across intake, design, production, and communication—under varying case conditions.
This article outlines a structured framework for evaluating outsourcing laboratories, focusing on three core dimensions: quality control discipline, communication structure, and consistency in execution.
Reliability as a Workflow Property, Not a Single Capability
A common misconception is that reliability is determined by technical skill alone. In practice, most laboratories can produce acceptable results under controlled conditions. The difference emerges when:
- Case volume increases
- Case complexity varies
- Input quality becomes inconsistent
A reliable partner maintains stable performance under these conditions. This requires not only technical capability but also structured processes that govern how cases are handled at every stage.
In dental outsourcing lab selection, the focus should shift from individual outputs to system behavior.
Intake Quality Control: The First Indicator of Reliability
The intake stage is the earliest point at which workflow stability can be assessed.
What a Reliable Lab Verifies at Intake
A structured intake process includes:
- Validation of required scan sets (preparation, antagonist, bite)
- Assessment of file compatibility across formats (e.g., STL, PLY, XML, DCM)
- Review of prescription completeness and clarity
- Identification of missing or inconsistent data
Cases that do not meet these criteria are not processed immediately. Instead, they are paused until sufficient information is provided.
Why Intake Discipline Matters
Labs that bypass intake validation may appear faster initially but introduce downstream inefficiencies:
- Interrupted design workflows
- Increased communication during processing
- Higher likelihood of remakes
A reliable laboratory enforces intake QC consistently, even if it delays individual cases. This approach stabilizes the overall workflow.
Communication Structure: From Informal Exchange to Defined Protocols
Communication is often underestimated in outsourcing relationships. However, it is one of the primary determinants of workflow efficiency.
Characteristics of Structured Communication
Reliable laboratories define:
- Standardized case submission formats
- Clear channels for file transfer and communication
- Documented case instructions and parameters
- Response protocols for clarification requests
These elements ensure that dental outsourcing lab selection is not dependent on informal or ad hoc communication.
Impact on Timeline Stability
When communication is structured:
- Cases proceed without repeated clarification
- Design teams operate with clear parameters
- Delays caused by misinterpretation are minimized
Conversely, unstructured communication leads to fragmented workflows and unpredictable turnaround times.
Design Consistency: Repeatability Across Cases
Consistency in CAD design is a key indicator of reliability. It reflects how well a laboratory standardizes its internal processes.
Indicators of Design Consistency
- Uniform margin handling across cases
- Consistent occlusal design protocols
- Stable application of thickness and material parameters
- Predictable anatomical outcomes
Consistency reduces variability, which is essential for maintaining efficiency at scale.
Risks of Inconsistent Design
When design approaches vary:
- Adjustments increase at the clinical stage
- Remake rates rise
- Workflow becomes less predictable
In dental outsourcing lab selection, consistency is often more valuable than peak performance on individual cases.
Alignment Between Design and Manufacturing
A reliable outsourcing laboratory does not treat design and production as separate functions. Instead, it ensures that both stages are aligned.
Design for Manufacturability
Design must account for:
- Material-specific constraints
- Minimum thickness requirements
- Production tolerances
If design decisions are not aligned with manufacturing capabilities, issues arise during fabrication.
Integrated Workflow Advantage
When design and production are coordinated:
- Cases transition smoothly between stages
- Adjustments during production are minimized
- Output matches design intent consistently
This integration is a critical factor in evaluating outsourcing partners.
Turnaround Time as a Measure of Process Stability
Turnaround time is often used as a primary selection criterion. However, its significance lies in consistency rather than speed.
What Reliable Turnaround Looks Like
- Defined timelines based on case complexity
- Predictable start points after intake validation
- Minimal variation across similar cases
Turnaround time should reflect a controlled process rather than reactive execution.
Factors Influencing Turnaround
Reliable laboratories structure their timelines based on:
- Case completeness
- Complexity and volume
- Workflow capacity and scheduling
For example, design timelines are typically adjusted based on case size and complexity rather than applied uniformly.
Case Tracking and Workflow Transparency
Transparency in workflow management is another key indicator of reliability.
Features of Transparent Systems
- Real-time case status tracking
- Visibility into design and production stages
- Shipment and delivery updates
These systems allow both laboratory and clinic to monitor progress without relying on manual follow-up.
Benefits for Workflow Control
- Reduced uncertainty in case handling
- Faster identification of issues
- Improved coordination between stages
Transparency supports accountability and enhances overall efficiency.
Handling Variability: A Core Test of Reliability
In real-world workflows, variability is unavoidable. Reliable laboratories are defined by how they manage it.
Sources of Variability
- Differences in scan quality
- Variations in case complexity
- Inconsistent prescription details
Structured Response to Variability
Reliable partners implement:
- Standardized intake criteria
- Flexible but controlled design protocols
- Clear communication for resolving discrepancies
This ensures that variability does not translate into workflow instability.
Scalability and Capacity Management
As case volume increases, the ability to scale becomes critical.
Indicators of Scalable Systems
- Ability to handle fluctuating case volumes
- Consistent performance under increased demand
- Structured allocation of design and production resources
Risks of Limited Scalability
- Bottlenecks during peak periods
- Delays due to capacity constraints
- Reduced consistency in output
In dental outsourcing lab selection, scalability determines whether a partner can support long-term growth.
Quality Control Beyond Final Inspection
Quality control is often associated with final inspection. In reliable workflows, it is distributed across multiple stages.
Multi-Level QC Structure
- Intake QC: Validating input data
- Design QC: Reviewing digital output
- Production QC: Verifying physical restorations
This layered approach reduces cumulative error and improves overall accuracy.
Impact on Workflow Efficiency
- Fewer remakes
- Reduced need for adjustments
- More predictable outcomes
Quality control, when applied consistently, becomes a driver of efficiency rather than a constraint.
Evaluating Risk in Outsourcing Partnerships
Selecting a laboratory also involves assessing operational risk.
Key Risk Factors
- Dependence on informal communication
- Lack of standardized processes
- Inconsistent turnaround performance
- Limited transparency in case handling
Risk Mitigation Through Structure
Reliable laboratories reduce risk by:
- Defining clear workflows
- Enforcing intake and QC protocols
- Maintaining consistent communication
This structured approach supports long-term collaboration.
A Practical Framework for Dental Outsourcing Lab Selection
Based on workflow considerations, a reliable laboratory can be evaluated across three core dimensions:
1. Input Control
- Does the lab enforce intake quality control?
- Are submission requirements clearly defined?
2. Process Stability
- Are design and production workflows standardized?
- Is turnaround time consistent across cases?
3. Output Consistency
- Are results repeatable across similar cases?
- Are remakes and adjustments minimized?
This framework shifts the focus from isolated capabilities to system-level performance.
Conclusion: Reliability Is Built on Process Discipline
Dental outsourcing lab selection is fundamentally a decision about workflow structure. A reliable laboratory is not defined by individual strengths but by its ability to maintain consistent performance across all stages of the process.
From intake validation and communication to design consistency and production alignment, each element contributes to overall reliability. Laboratories that enforce structured workflows, maintain transparency, and manage variability effectively provide a more stable foundation for long-term collaboration.
In digital dental workflows, reliability is not an outcome—it is a property of the system that produces it.
In digital dental production, the decision between maintaining an internal CAD design team and working with an external partner is often framed as a question of control versus cost. In practice, the more relevant comparison is operational: how each model performs within a structured workflow and how it scales under variable demand.
In-house vs outsourced dental CAD is not a binary choice of capability. Both models can produce technically accurate designs. The difference lies in how each approach manages workflow continuity, absorbs variability, and maintains consistency across case volumes and complexity levels.
This article evaluates in-house and outsourced CAD design from a workflow perspective, focusing on intake discipline, processing stability, communication structure, and scalability.
Before comparing models, it is important to position CAD design correctly within the workflow. Design is not an isolated activity; it is a central node connecting:
Any disruption at this stage affects both upstream and downstream processes. Therefore, the evaluation of in-house vs outsourced dental CAD should focus on how each model maintains stability at this critical node.
Internal teams often operate in close proximity to case intake. This allows:
However, this flexibility can introduce inconsistency. Designers may proceed with partial information, relying on assumptions to maintain speed.
External workflows typically enforce stricter intake validation:
This approach ensures that only validated cases enter the design queue.
From a workflow perspective, outsourcing emphasizes input discipline, while in-house models often prioritize immediate processing. The former reduces downstream variability, while the latter may increase it.
In internal environments:
This is particularly evident in high-volume settings where case complexity varies.
In outsourced environments:
This separation reduces mid-process interruptions and supports continuous workflow execution.
In in-house vs outsourced dental CAD, the key difference lies in how interruptions are handled:
This structural difference has a direct impact on efficiency and predictability.
Turnaround time is often used as a comparison metric, but its interpretation differs between models.
While individual cases may be processed quickly, overall consistency may fluctuate.
Design timelines are structured according to complexity and completeness rather than immediate availability.
In-house models emphasize responsiveness, while outsourced models emphasize consistency. The choice depends on whether the workflow prioritizes flexibility or predictability.
Internal teams may develop individual design habits:
While this allows flexibility, it can lead to variability across cases.
Outsourced workflows typically rely on:
This reduces variability and supports repeatable outcomes.
Consistency in design reduces the need for:
From a workflow perspective, standardization supports scalability.
Communication within internal teams is often informal:
While efficient for small teams, this approach may not scale effectively.
External workflows rely on structured communication:
Case tracking systems may be used to monitor progress and updates.
Structured communication reduces ambiguity and supports consistent processing, especially in high-volume environments.
Scaling internal design capacity requires:
This process is resource-intensive and may lag behind demand.
Outsourcing allows:
This enables more immediate scalability without structural changes.
In in-house vs outsourced dental CAD, scalability is a key differentiator:
Internal teams may have:
This can be advantageous for highly customized restorations.
Outsourced partners often:
Complex cases may require more structured input to achieve desired outcomes.
The effectiveness of either model depends on how well complexity is managed through communication and process control.
Quality control is often integrated within the design process:
This approach relies on individual consistency.
Outsourced workflows typically include:
This layered approach reduces cumulative errors.
Structured QC reduces rework and supports more predictable outcomes across cases.
Each model distributes risk differently. The choice depends on whether the workflow prioritizes internal control or external flexibility.
In practice, many laboratories adopt a hybrid approach:
This allows:
From a workflow perspective, hybrid models aim to combine the strengths of both approaches.
When evaluating in-house vs outsourced dental CAD, the decision should be based on workflow priorities rather than assumptions.
The comparison between in-house and outsourced CAD design is not about which model is inherently superior. It is about how each model supports the overall workflow.
In-house vs outsourced dental CAD should be evaluated based on:
In digital dental production, efficiency is achieved not by optimizing individual steps, but by maintaining continuity across the entire workflow. The model that best supports this continuity will deliver the most predictable and scalable results.
In-house vs outsourced dental CAD is not a binary choice of capability. Both models can produce technically accurate designs. The difference lies in how each approach manages workflow continuity, absorbs variability, and maintains consistency across case volumes and complexity levels.
This article evaluates in-house and outsourced CAD design from a workflow perspective, focusing on intake discipline, processing stability, communication structure, and scalability.
Understanding CAD Design as a Workflow Node
Before comparing models, it is important to position CAD design correctly within the workflow. Design is not an isolated activity; it is a central node connecting:
- Case intake and data validation
- Occlusal and anatomical design decisions
- Manufacturing preparation and output
Any disruption at this stage affects both upstream and downstream processes. Therefore, the evaluation of in-house vs outsourced dental CAD should focus on how each model maintains stability at this critical node.
Intake Dependency: How Each Model Handles Input Variability
In-House CAD Design
Internal teams often operate in close proximity to case intake. This allows:
- Immediate access to submitted data
- Faster informal communication with clinicians
- Greater flexibility in handling incomplete cases
However, this flexibility can introduce inconsistency. Designers may proceed with partial information, relying on assumptions to maintain speed.
Outsourced CAD Design
External workflows typically enforce stricter intake validation:
- Cases are reviewed for completeness before design begins
- Missing information results in case pausing
- Standardized submission requirements are applied
This approach ensures that only validated cases enter the design queue.
Workflow Implication
From a workflow perspective, outsourcing emphasizes input discipline, while in-house models often prioritize immediate processing. The former reduces downstream variability, while the latter may increase it.
Workflow Continuity and Interruption Management
In-House Model
In internal environments:
- Designers often manage multiple roles, including communication and troubleshooting
- Interruptions occur when clarification is needed
- Workflow can become fragmented due to task switching
This is particularly evident in high-volume settings where case complexity varies.
Outsourced Model
In outsourced environments:
- Design workflows are typically segmented from intake and communication
- Only validated cases are processed
- Designers operate within uninterrupted queues
This separation reduces mid-process interruptions and supports continuous workflow execution.
Workflow Comparison
In in-house vs outsourced dental CAD, the key difference lies in how interruptions are handled:
- In-house: interruptions are absorbed within the design process
- Outsourced: interruptions are filtered out at intake
This structural difference has a direct impact on efficiency and predictability.
Turnaround Time: Stability vs Responsiveness
Turnaround time is often used as a comparison metric, but its interpretation differs between models.
In-House Turnaround Characteristics
- Potential for rapid response on individual cases
- Flexibility to prioritize urgent cases immediately
- Variability depending on team workload
While individual cases may be processed quickly, overall consistency may fluctuate.
Outsourced Turnaround Characteristics
- Defined processing timelines based on case type and volume
- Turnaround begins after case validation
- Greater consistency across cases
Design timelines are structured according to complexity and completeness rather than immediate availability.
Workflow Comparison
In-house models emphasize responsiveness, while outsourced models emphasize consistency. The choice depends on whether the workflow prioritizes flexibility or predictability.
Design Consistency and Standardization
In-House Variability
Internal teams may develop individual design habits:
- Differences in margin interpretation
- Variations in occlusal design
- Inconsistent parameter application
While this allows flexibility, it can lead to variability across cases.
Outsourced Standardization
Outsourced workflows typically rely on:
- Defined design protocols
- Standardized parameter settings
- Consistent quality control processes
This reduces variability and supports repeatable outcomes.
Impact on Workflow
Consistency in design reduces the need for:
- Adjustments during production
- Remakes due to design discrepancies
- Case-specific troubleshooting
From a workflow perspective, standardization supports scalability.
Communication Structure and Its Effect on Efficiency
In-House Communication
Communication within internal teams is often informal:
- Direct interaction between clinicians and designers
- Faster clarification for simple issues
- Potential lack of documentation
While efficient for small teams, this approach may not scale effectively.
Outsourced Communication
External workflows rely on structured communication:
- Defined submission formats
- Documented case instructions
- Formal feedback loops
Case tracking systems may be used to monitor progress and updates.
Workflow Implication
Structured communication reduces ambiguity and supports consistent processing, especially in high-volume environments.
Scalability Under Increasing Case Volume
In-House Scalability
Scaling internal design capacity requires:
- Hiring and training additional designers
- Expanding infrastructure
- Managing team coordination
This process is resource-intensive and may lag behind demand.
Outsourced Scalability
Outsourcing allows:
- Flexible allocation of design capacity
- Handling of peak volumes without internal expansion
- Distribution of workload across larger teams
This enables more immediate scalability without structural changes.
Workflow Comparison
In in-house vs outsourced dental CAD, scalability is a key differentiator:
- In-house: capacity is fixed and grows incrementally
- Outsourced: capacity is variable and adjusts to demand
Handling Complex Cases and Specialized Requirements
In-House Strengths
Internal teams may have:
- Direct familiarity with specific clinicians’ preferences
- Greater flexibility in handling unique cases
- Immediate access to contextual information
This can be advantageous for highly customized restorations.
Outsourced Capabilities
Outsourced partners often:
- Handle a wide range of case types
- Apply standardized approaches to complex workflows
- Require clear communication for customization
Complex cases may require more structured input to achieve desired outcomes.
Workflow Consideration
The effectiveness of either model depends on how well complexity is managed through communication and process control.
Quality Control Integration
In-House QC
Quality control is often integrated within the design process:
- Designers self-check their work
- Additional QC steps may vary depending on workload
This approach relies on individual consistency.
Outsourced QC
Outsourced workflows typically include:
- Dedicated intake QC
- Design-level validation
- Pre-production checks
This layered approach reduces cumulative errors.
Impact on Workflow
Structured QC reduces rework and supports more predictable outcomes across cases.
Risk Distribution and Dependency
In-House Risk Profile
- Dependence on a limited number of designers
- Risk of workflow disruption due to staff availability
- Internal bottlenecks during peak demand
Outsourced Risk Profile
- Dependence on external coordination
- Potential delays if communication is incomplete
- Reduced risk of capacity limitations
Workflow Perspective
Each model distributes risk differently. The choice depends on whether the workflow prioritizes internal control or external flexibility.
Hybrid Models: Combining In-House and Outsourcing
In practice, many laboratories adopt a hybrid approach:
- Core cases handled internally
- Overflow and standardized cases outsourced
This allows:
- Retention of internal expertise
- Flexible scaling during peak periods
- Balanced control and efficiency
From a workflow perspective, hybrid models aim to combine the strengths of both approaches.
Decision Framework Based on Workflow Priorities
When evaluating in-house vs outsourced dental CAD, the decision should be based on workflow priorities rather than assumptions.
When In-House May Be Preferred
- Low to moderate case volume
- High need for customization
- Strong internal design team
When Outsourcing May Be Preferred
- High or variable case volume
- Need for consistent turnaround
- Focus on workflow standardization
When Hybrid Models Are Effective
- Mixed case complexity
- Fluctuating demand
- Need for both flexibility and control
Conclusion: Workflow Structure Determines the Better Model
The comparison between in-house and outsourced CAD design is not about which model is inherently superior. It is about how each model supports the overall workflow.
In-house vs outsourced dental CAD should be evaluated based on:
- How well input variability is managed
- How consistently cases move through the design stage
- How effectively the system scales with demand
In digital dental production, efficiency is achieved not by optimizing individual steps, but by maintaining continuity across the entire workflow. The model that best supports this continuity will deliver the most predictable and scalable results.
Turnaround time is one of the most frequently discussed metrics in digital dental workflows. It is often interpreted as a simple measure of speed—how fast a case can be designed and delivered. In practice, however, dental CAD turnaround time is not defined by a single step or capability. It is the outcome of multiple interdependent variables across the entire workflow.
From a laboratory perspective, turnaround time is a function of workflow stability rather than isolated efficiency. Cases move predictably when input quality is controlled, communication is structured, and design processes are aligned with production requirements. When these conditions are not met, delays occur—even in systems with high technical capacity.
This article examines what actually determines turnaround time in dental CAD design services, focusing on the underlying workflow logic rather than speed-based assumptions.
A common misconception is that turnaround time starts when a case is submitted. In structured workflows, this is not the case.
Before design begins, cases must be validated for:
If any required information is missing, the case is paused until it is resolved.
This means that dental CAD turnaround time effectively begins only after:
Cases that enter the workflow without full validation often experience hidden delays later, making their total processing time longer despite earlier submission.
Not all cases require the same level of design effort. Complexity is one of the primary determinants of turnaround time.
Turnaround time must be structured according to complexity rather than standardized across all cases. In practice, design timelines vary based on case type and size.
One of the most critical factors affecting dental CAD turnaround time is the quality of the submitted data.
When scan data is:
design can proceed without interruption. This leads to:
When data is incomplete or unclear:
These interruptions extend the total turnaround time, even if the actual design step is relatively short.
Turnaround time is closely tied to how efficiently information flows between the clinic and the laboratory.
Effective communication ensures that:
When dental CAD turnaround time is affected by communication issues, delays typically occur due to:
These delays are often more significant than the time required for actual design execution.
Design capacity is finite, and cases must be managed within a queue.
In structured workflows:
In unstructured workflows:
Interrupted workflows reduce efficiency and increase total processing time, even if individual design tasks are short.
Standardization within CAD design processes contributes significantly to stable turnaround times.
When design parameters are standardized:
Standardization minimizes the need for:
This improves efficiency and supports consistent dental CAD turnaround time across different case types.
Although turnaround time is often associated with CAD design, it is influenced by how well design integrates with production.
Designs must account for:
If designs are not aligned with manufacturing constraints:
When design and manufacturing are aligned, cases move seamlessly from one stage to the next, reducing total turnaround time.
Turnaround time is also affected by how cases are prioritized within the workflow.
Cases may be categorized based on:
Structured workflows allow for:
When priorities are clearly defined, dental CAD turnaround time can be managed more effectively across different case types.
In outsourcing environments, operational coverage can influence turnaround time.
Laboratories operating across multiple time zones can:
This enables a more continuous workflow, reducing delays caused by time gaps between stages.
However, this benefit is only realized when input data and communication are complete.
Quality control is often perceived as an additional step that increases processing time. In practice, it defines overall efficiency.
Although QC adds time at specific stages, it reduces total turnaround time by preventing rework and delays.
One of the challenges in evaluating dental CAD turnaround time is distinguishing between visible and hidden delays.
In many cases, hidden delays account for a significant portion of total turnaround time.
Different laboratories adopt different strategies for managing turnaround.
The second approach typically results in more stable and reliable turnaround performance.
Several factors influencing turnaround time are not fully controllable:
However, structured workflows mitigate these variables by:
Dental CAD turnaround time is not determined by how quickly a design can be completed in isolation. It is the result of how effectively the entire workflow is structured—from intake validation and communication to design execution and production alignment.
Focusing solely on speed overlooks the underlying factors that create delays. By addressing input quality, communication clarity, workflow continuity, and quality control, laboratories and clinics can achieve more predictable and efficient turnaround times.
In digital dental workflows, consistency—not speed alone—is the defining characteristic of reliable turnaround performance.
From a laboratory perspective, turnaround time is a function of workflow stability rather than isolated efficiency. Cases move predictably when input quality is controlled, communication is structured, and design processes are aligned with production requirements. When these conditions are not met, delays occur—even in systems with high technical capacity.
This article examines what actually determines turnaround time in dental CAD design services, focusing on the underlying workflow logic rather than speed-based assumptions.
Turnaround Time Begins After Case Validation, Not Submission
A common misconception is that turnaround time starts when a case is submitted. In structured workflows, this is not the case.
Intake Validation as the Starting Point
Before design begins, cases must be validated for:
- Completeness of scan data (preparation, antagonist, bite)
- File compatibility and integrity
- Clarity of prescription and design parameters
If any required information is missing, the case is paused until it is resolved.
Impact on Turnaround Measurement
This means that dental CAD turnaround time effectively begins only after:
- All required data is confirmed
- The case is ready for uninterrupted processing
Cases that enter the workflow without full validation often experience hidden delays later, making their total processing time longer despite earlier submission.
Case Complexity as a Structural Variable
Not all cases require the same level of design effort. Complexity is one of the primary determinants of turnaround time.
Simple vs. Complex Cases
- Single-unit restorations: Typically require less design time due to limited anatomical and occlusal considerations
- Multi-unit bridges: Require connector design, occlusal coordination, and structural balancing
- Implant restorations: Involve additional variables such as interface alignment and emergence profile
- Full-arch cases: Require extended planning, articulation, and design verification
Implications for Workflow Planning
Turnaround time must be structured according to complexity rather than standardized across all cases. In practice, design timelines vary based on case type and size.
Input Data Quality and Its Direct Impact on Processing Time
One of the most critical factors affecting dental CAD turnaround time is the quality of the submitted data.
Effects of High-Quality Input
When scan data is:
- Complete
- Clear
- Structurally consistent
design can proceed without interruption. This leads to:
- Continuous workflow
- Minimal need for clarification
- Predictable design timelines
Effects of Low-Quality Input
When data is incomplete or unclear:
- Designers must request additional information
- Cases are paused mid-process
- Redesign or correction may be required
These interruptions extend the total turnaround time, even if the actual design step is relatively short.
Case Communication and Its Influence on Workflow Continuity
Turnaround time is closely tied to how efficiently information flows between the clinic and the laboratory.
Role of Clear Communication
Effective communication ensures that:
- Design parameters are understood from the beginning
- Special instructions are incorporated correctly
- Clarification is minimized during processing
Impact of Communication Gaps
When dental CAD turnaround time is affected by communication issues, delays typically occur due to:
- Waiting for responses to clarification requests
- Misinterpretation of incomplete instructions
- Rework caused by incorrect assumptions
These delays are often more significant than the time required for actual design execution.
Workflow Queue Management and Case Flow
Design capacity is finite, and cases must be managed within a queue.
Continuous vs. Interrupted Flow
In structured workflows:
- Cases enter the queue only after validation
- Designers process cases without interruption
- Output remains consistent
In unstructured workflows:
- Cases enter the queue with incomplete data
- Designers must pause and switch between tasks
- Workflow becomes fragmented
Effect on Turnaround Time
Interrupted workflows reduce efficiency and increase total processing time, even if individual design tasks are short.
Design Standardization and Its Role in Predictability
Standardization within CAD design processes contributes significantly to stable turnaround times.
Consistent Design Protocols
When design parameters are standardized:
- Designers spend less time making case-by-case adjustments
- Output becomes more predictable
- Variability between cases is reduced
Reduced Decision Overhead
Standardization minimizes the need for:
- Reinterpretation of clinical intent
- Custom adjustments for each case
This improves efficiency and supports consistent dental CAD turnaround time across different case types.
The Relationship Between Design and Manufacturing Alignment
Although turnaround time is often associated with CAD design, it is influenced by how well design integrates with production.
Design for Manufacturability
Designs must account for:
- Material limitations
- Minimum thickness requirements
- Production tolerances
If designs are not aligned with manufacturing constraints:
- Adjustments are required before production
- Cases may need to be redesigned
- Production schedules are delayed
Integrated Workflow Impact
When design and manufacturing are aligned, cases move seamlessly from one stage to the next, reducing total turnaround time.
Priority Handling and Case Segmentation
Turnaround time is also affected by how cases are prioritized within the workflow.
Case Segmentation
Cases may be categorized based on:
- Urgency
- Complexity
- Volume
Priority Allocation
Structured workflows allow for:
- Expedited handling of urgent cases
- Standard processing for routine cases
- Flexible allocation of resources
When priorities are clearly defined, dental CAD turnaround time can be managed more effectively across different case types.
Time Zone and Operational Coverage
In outsourcing environments, operational coverage can influence turnaround time.
Extended Processing Windows
Laboratories operating across multiple time zones can:
- Process cases outside the clinic’s working hours
- Reduce idle time between submission and design initiation
Impact on Workflow Continuity
This enables a more continuous workflow, reducing delays caused by time gaps between stages.
However, this benefit is only realized when input data and communication are complete.
Quality Control as a Time-Defining Factor
Quality control is often perceived as an additional step that increases processing time. In practice, it defines overall efficiency.
Pre-Design QC
- Ensures that only complete cases enter the workflow
- Prevents interruptions during design
Post-Design QC
- Identifies issues before production
- Reduces the likelihood of remakes
Net Effect on Turnaround Time
Although QC adds time at specific stages, it reduces total turnaround time by preventing rework and delays.
Hidden Delays vs. Visible Processing Time
One of the challenges in evaluating dental CAD turnaround time is distinguishing between visible and hidden delays.
Visible Time
- Time spent on design
- Defined processing windows
Hidden Time
- Waiting for missing information
- Rework due to errors
- Communication delays
In many cases, hidden delays account for a significant portion of total turnaround time.
Two Approaches to Managing Turnaround Time
Different laboratories adopt different strategies for managing turnaround.
Speed-Focused Approach
- Emphasis on rapid design execution
- Minimal intake validation
- Higher risk of interruptions and rework
Workflow-Focused Approach
- Emphasis on structured intake and communication
- Continuous, uninterrupted processing
- More predictable outcomes
The second approach typically results in more stable and reliable turnaround performance.
Limitations and Practical Constraints
Several factors influencing turnaround time are not fully controllable:
- Variability in scan quality
- Differences in case complexity
- Response time from clinics
However, structured workflows mitigate these variables by:
- Defining clear intake requirements
- Standardizing communication
- Maintaining consistent design protocols
Conclusion: Turnaround Time as a System Outcome
Dental CAD turnaround time is not determined by how quickly a design can be completed in isolation. It is the result of how effectively the entire workflow is structured—from intake validation and communication to design execution and production alignment.
Focusing solely on speed overlooks the underlying factors that create delays. By addressing input quality, communication clarity, workflow continuity, and quality control, laboratories and clinics can achieve more predictable and efficient turnaround times.
In digital dental workflows, consistency—not speed alone—is the defining characteristic of reliable turnaround performance.

In digital dental workflows, delays are often attributed to design complexity or production capacity. However, from a laboratory perspective, one of the most consistent sources of inefficiency is less technical: unclear or incomplete communication between the clinic and the lab.
Dental lab case communication directly influences how quickly and accurately a case moves from intake to design, through production, and toward delivery. When communication is structured and complete, workflows remain continuous. When it is fragmented or ambiguous, delays emerge at multiple stages—often in ways that are not immediately visible.
This article analyzes how communication affects workflow timelines in dental lab outsourcing and how structured communication reduces interruptions across the entire process.
In many workflows, communication is treated as a secondary activity—something that occurs when issues arise. In practice, communication is a core operational variable that determines whether a case can proceed without interruption.
At each stage of the workflow, communication defines:
If dental lab case communication is incomplete at the beginning, the workflow becomes reactive. Designers and technicians must pause, clarify, and reinterpret information, leading to fragmented timelines.
Communication influences multiple control points within the workflow. Delays typically do not occur at a single stage but accumulate across transitions.
At intake, communication determines whether the case is complete and ready for processing.
Required elements include:
If any of these elements are unclear or missing, the case cannot proceed. Instead, it must be paused until clarification is received.
During CAD design, unclear communication leads to:
Each assumption introduces risk and may require correction later in the workflow.
At the production stage, communication gaps can result in:
These issues often require rework, extending the total turnaround time.
One of the challenges in managing dental lab case communication is that its impact on timelines is often indirect.
Visible delays include:
Hidden delays include:
While visible delays are easier to track, hidden delays often have a greater cumulative impact on workflow efficiency.
A key determinant of workflow speed is not how quickly a case is processed, but how completely it is defined at the start.
When communication is clear and complete:
When communication is incomplete:
Structured workflows prioritize completeness over immediate processing to maintain overall efficiency.
To reduce variability, many laboratories implement structured communication protocols.
Protocols typically define:
This ensures that all cases entering the workflow meet consistent criteria.
Clear channels are established for:
This reduces delays caused by fragmented or informal communication.
Effective dental lab case communication includes not only initial submission but also ongoing feedback.
When issues are identified:
If information is provided promptly, the case can continue within the same processing cycle. If not, it may be deferred to the next cycle.
Over time, consistent feedback leads to:
This transforms communication from a reactive process into a proactive system.
Turnaround time is often treated as a fixed metric. In reality, it is highly dependent on communication efficiency.
In structured workflows:
In unstructured workflows:
Clear dental lab case communication enables consistent turnaround by reducing variability.
Not all cases require the same level of urgency. Effective communication allows for proper prioritization.
Clinics may specify:
When priorities are clearly communicated:
Without clear prioritization, urgent cases may be delayed, and standard cases may be unnecessarily expedited.
Modern outsourcing workflows often include digital systems for managing communication and case tracking.
These systems provide a structured framework for dental lab case communication, reducing reliance on manual follow-up.
Understanding where communication fails helps identify how delays are introduced.
Effect: Design cannot proceed or requires assumptions.
Effect: Occlusal and margin inaccuracies.
Effect: Cases are postponed, affecting overall workflow.
Different laboratories adopt different approaches to communication.
The second approach supports more stable and predictable workflows.
There is often a perceived trade-off between speed and thorough communication.
From a workflow perspective, investing in communication upfront reduces total processing time.
While structured communication improves efficiency, it requires:
Without these elements, communication protocols may become ineffective.
However, when properly implemented, they significantly reduce workflow variability.
In dental lab outsourcing, dental lab case communication is a primary determinant of workflow efficiency and timeline stability.
Clear, structured communication ensures that cases move through intake, design, and production without interruption. It reduces the need for clarification, minimizes rework, and supports predictable turnaround times.
For laboratories and clinics seeking to optimize digital workflows, improving communication is not an optional enhancement—it is a fundamental requirement for consistent and efficient case execution.
Dental lab case communication directly influences how quickly and accurately a case moves from intake to design, through production, and toward delivery. When communication is structured and complete, workflows remain continuous. When it is fragmented or ambiguous, delays emerge at multiple stages—often in ways that are not immediately visible.
This article analyzes how communication affects workflow timelines in dental lab outsourcing and how structured communication reduces interruptions across the entire process.
Communication as a Workflow Variable, Not a Support Function
In many workflows, communication is treated as a secondary activity—something that occurs when issues arise. In practice, communication is a core operational variable that determines whether a case can proceed without interruption.
At each stage of the workflow, communication defines:
- What the lab understands about the case
- Whether the provided data is sufficient
- How decisions are made during design and production
If dental lab case communication is incomplete at the beginning, the workflow becomes reactive. Designers and technicians must pause, clarify, and reinterpret information, leading to fragmented timelines.
Where Communication Directly Impacts Timeline
Communication influences multiple control points within the workflow. Delays typically do not occur at a single stage but accumulate across transitions.
Intake Stage: Defining Case Readiness
At intake, communication determines whether the case is complete and ready for processing.
Required elements include:
- Clear prescription details
- Defined restoration type and material
- Complete scan set (preparation, antagonist, bite)
- Any specific instructions or constraints
If any of these elements are unclear or missing, the case cannot proceed. Instead, it must be paused until clarification is received.
Design Stage: Reducing Interpretation
During CAD design, unclear communication leads to:
- Assumptions about occlusion or margin placement
- Inconsistent anatomical design
- Increased variability between cases
Each assumption introduces risk and may require correction later in the workflow.
Production Stage: Preventing Rework
At the production stage, communication gaps can result in:
- Incorrect material selection
- Misalignment between design intent and manufacturing parameters
- Reproduction of flawed designs
These issues often require rework, extending the total turnaround time.
The Hidden Nature of Communication-Related Delays
One of the challenges in managing dental lab case communication is that its impact on timelines is often indirect.
Visible vs. Hidden Delays
Visible delays include:
- Waiting for missing files
- Explicit requests for clarification
Hidden delays include:
- Designers working with incomplete information
- Adjustments during production
- Increased chairside correction
While visible delays are easier to track, hidden delays often have a greater cumulative impact on workflow efficiency.
Case Completeness and Its Relationship to Timeline Stability
A key determinant of workflow speed is not how quickly a case is processed, but how completely it is defined at the start.
Complete Cases
When communication is clear and complete:
- Design can begin immediately
- No mid-process interruptions occur
- Turnaround times remain predictable
Incomplete Cases
When communication is incomplete:
- Cases are paused or delayed
- Design workflows are interrupted
- Production schedules become unstable
Structured workflows prioritize completeness over immediate processing to maintain overall efficiency.
Communication Protocols as a Workflow Control Mechanism
To reduce variability, many laboratories implement structured communication protocols.
Standardized Case Submission
Protocols typically define:
- Required files and formats
- Mandatory prescription fields
- Minimum data quality thresholds
This ensures that all cases entering the workflow meet consistent criteria.
Defined Communication Channels
Clear channels are established for:
- Case submission (email, portal, file transfer systems)
- Clarification requests
- Status updates
This reduces delays caused by fragmented or informal communication.
Feedback Loops and Their Role in Reducing Delays
Effective dental lab case communication includes not only initial submission but also ongoing feedback.
Handling Missing or Incomplete Information
When issues are identified:
- The lab communicates specific deficiencies
- The clinic provides updated data
- The case is revalidated before proceeding
If information is provided promptly, the case can continue within the same processing cycle. If not, it may be deferred to the next cycle.
Long-Term Improvement
Over time, consistent feedback leads to:
- Improved submission quality
- Fewer interruptions
- More stable timelines
This transforms communication from a reactive process into a proactive system.
The Relationship Between Communication and Turnaround Time
Turnaround time is often treated as a fixed metric. In reality, it is highly dependent on communication efficiency.
Structured Turnaround vs. Variable Turnaround
In structured workflows:
- Turnaround begins only after case validation
- Timelines are defined based on case complexity
- Communication delays are minimized
In unstructured workflows:
- Turnaround is interrupted by clarification requests
- Timelines vary unpredictably
- Delays accumulate across stages
Clear dental lab case communication enables consistent turnaround by reducing variability.
Communication and Case Prioritization
Not all cases require the same level of urgency. Effective communication allows for proper prioritization.
Defining Case Priority
Clinics may specify:
- Urgent cases requiring expedited processing
- Standard cases following normal timelines
- Complex cases requiring extended design time
Impact on Workflow Allocation
When priorities are clearly communicated:
- Resources can be allocated efficiently
- Bottlenecks are avoided
- Deadlines are met more consistently
Without clear prioritization, urgent cases may be delayed, and standard cases may be unnecessarily expedited.
Integration with Case Management Systems
Modern outsourcing workflows often include digital systems for managing communication and case tracking.
Features of Integrated Systems
- Centralized case information
- Real-time status updates
- Tracking of design and production stages
- Shipment and delivery visibility
These systems provide a structured framework for dental lab case communication, reducing reliance on manual follow-up.
Benefits for Workflow Transparency
- Improved visibility into case progress
- Reduced uncertainty for both lab and clinic
- Faster response to issues
Common Communication Breakdowns and Their Effects
Understanding where communication fails helps identify how delays are introduced.
Incomplete Prescriptions
- Missing material or design parameters
- Ambiguity in restoration type
Effect: Design cannot proceed or requires assumptions.
Unclear Scan Data Context
- Lack of indication for margin location
- Missing bite registration
Effect: Occlusal and margin inaccuracies.
Delayed Responses
- Slow clarification from clinic
- Lack of defined response timelines
Effect: Cases are postponed, affecting overall workflow.
Two Approaches to Communication in Outsourcing
Different laboratories adopt different approaches to communication.
Reactive Communication
- Issues addressed only when they arise
- Informal or inconsistent communication channels
- High variability in timelines
Structured Communication
- Defined protocols and requirements
- Proactive validation at intake
- Continuous feedback and tracking
The second approach supports more stable and predictable workflows.
Balancing Communication Efficiency and Workflow Speed
There is often a perceived trade-off between speed and thorough communication.
Minimal Communication Approach
- Faster initial processing
- Increased risk of errors
- Higher likelihood of rework
Structured Communication Approach
- Additional time spent at intake
- Reduced need for mid-process clarification
- More predictable overall timelines
From a workflow perspective, investing in communication upfront reduces total processing time.
Limitations and Practical Considerations
While structured communication improves efficiency, it requires:
- Clear guidelines for case submission
- Consistent adherence by both lab and clinic
- Efficient communication channels
Without these elements, communication protocols may become ineffective.
However, when properly implemented, they significantly reduce workflow variability.
Conclusion: Communication as a Determinant of Workflow Predictability
In dental lab outsourcing, dental lab case communication is a primary determinant of workflow efficiency and timeline stability.
Clear, structured communication ensures that cases move through intake, design, and production without interruption. It reduces the need for clarification, minimizes rework, and supports predictable turnaround times.
For laboratories and clinics seeking to optimize digital workflows, improving communication is not an optional enhancement—it is a fundamental requirement for consistent and efficient case execution.
In digital dental workflows, most discussions around accuracy and efficiency focus on CAD design or manufacturing precision. However, from a laboratory perspective, the most decisive stage occurs earlier—at case intake. Before any design work begins, the quality, completeness, and consistency of submitted data determine whether the workflow will proceed smoothly or encounter delays, rework, and variability.
Dental case intake quality control is not an administrative step. It is a technical validation process that defines whether a case is ready for design. When intake is structured and disciplined, downstream processes become predictable. When intake is inconsistent, even highly skilled design and production teams are constrained by incomplete or inaccurate input.
This article examines why intake QC is critical, what it involves in practice, and how it directly impacts workflow stability.
In a digital environment, design does not begin when a file is opened in CAD software. It begins when the case is received and evaluated.
At intake, multiple variables converge:
If any of these variables are incomplete or inconsistent, the design process cannot proceed reliably.
A structured dental case intake quality control process ensures that all required inputs are validated before design begins, preventing the need for interpretation or assumption later in the workflow.
Effective intake QC is not a superficial check. It is a systematic evaluation of whether the case contains all necessary information for accurate design and manufacturing.
For crown and bridge cases, this typically includes:
Missing any of these elements compromises the ability to establish occlusion, margin placement, or spatial relationships.
Digital workflows involve multiple file types, including:
A structured intake process ensures that all files are readable and compatible with the design environment.
Design cannot proceed without defined parameters such as:
Incomplete prescriptions force designers to make assumptions, increasing variability in outcomes.
In high-volume environments, there may be pressure to begin design immediately upon receiving a case. However, proceeding without full validation introduces compounding inefficiencies.
When intake QC is enforced:
If information cannot be provided promptly, cases are typically deferred to the next processing cycle.
While this approach may delay individual cases, it prevents:
From a system perspective, enforcing intake QC reduces total turnaround time across all cases.
When dental case intake quality control is not applied consistently, errors propagate through the workflow.
These issues are often more costly to resolve than the time saved by skipping intake QC.
From a workflow perspective, intake QC functions as a bottleneck control mechanism.
By validating cases before design:
When only validated cases enter the design queue:
This transforms the workflow from reactive to controlled.
Turnaround time is often misunderstood as a measure of speed. In practice, it is a measure of consistency.
In disciplined workflows:
For example, design timelines may vary depending on case size and complexity, but only after the case is confirmed to be complete.
Without intake QC, delays occur later in the process:
These delays are less visible but more disruptive.
Intake QC is closely tied to communication between clinics and laboratories.
Effective intake processes define:
This reduces ambiguity and ensures that both parties operate within the same framework.
When issues are identified:
Over time, this improves submission quality and reduces intake errors.
Not all cases are submitted with the same level of completeness or quality. Variability is inevitable due to differences in:
A structured dental case intake quality control process mitigates this variability by:
This creates a stable foundation for design and production.
In high-volume environments, not all cases require the same level of urgency.
During intake, cases can be categorized based on:
This allows laboratories to:
Without intake QC, prioritization becomes reactive rather than planned.
Modern workflows often incorporate digital tools for case tracking and management.
Some systems provide shared dashboards or tracking links, enabling both laboratory and clinic to monitor case progress.
This integration improves:
Different laboratories approach intake in different ways.
The second approach leads to greater overall efficiency, despite appearing slower at the initial stage.
While intake QC improves workflow stability, it requires:
Without these elements, intake QC may become a bottleneck rather than a control mechanism.
However, when implemented correctly, it functions as a filter that stabilizes the entire workflow.
In digital dental workflows, dental case intake quality control is the foundation upon which all subsequent stages depend.
By ensuring that only complete, consistent, and compatible data enters the design process, intake QC reduces variability, prevents downstream errors, and supports predictable turnaround times.
For laboratories and clinics aiming to optimize efficiency and reduce rework, the focus should not begin at design or production, but at intake—where workflow stability is first established.
Dental case intake quality control is not an administrative step. It is a technical validation process that defines whether a case is ready for design. When intake is structured and disciplined, downstream processes become predictable. When intake is inconsistent, even highly skilled design and production teams are constrained by incomplete or inaccurate input.
This article examines why intake QC is critical, what it involves in practice, and how it directly impacts workflow stability.
Intake as the True Starting Point of the Digital Workflow
In a digital environment, design does not begin when a file is opened in CAD software. It begins when the case is received and evaluated.
At intake, multiple variables converge:
- Scan data quality (preparation, antagonist, bite)
- File compatibility and integrity
- Prescription clarity
- Restoration parameters and material selection
If any of these variables are incomplete or inconsistent, the design process cannot proceed reliably.
A structured dental case intake quality control process ensures that all required inputs are validated before design begins, preventing the need for interpretation or assumption later in the workflow.
What Intake Quality Control Actually Verifies
Effective intake QC is not a superficial check. It is a systematic evaluation of whether the case contains all necessary information for accurate design and manufacturing.
1. Completeness of Scan Data
For crown and bridge cases, this typically includes:
- Preparation scan
- Antagonist scan
- Bite registration
Missing any of these elements compromises the ability to establish occlusion, margin placement, or spatial relationships.
2. File Format and Compatibility
Digital workflows involve multiple file types, including:
- STL and PLY for geometry
- XML or DCM for additional data
- Other formats depending on scanner systems
A structured intake process ensures that all files are readable and compatible with the design environment.
3. Prescription and Parameter Clarity
Design cannot proceed without defined parameters such as:
- Restoration type
- Material selection
- Thickness requirements
- Special instructions
Incomplete prescriptions force designers to make assumptions, increasing variability in outcomes.
Why Cases Should Not Proceed Without Complete Intake Data
In high-volume environments, there may be pressure to begin design immediately upon receiving a case. However, proceeding without full validation introduces compounding inefficiencies.
Immediate vs. Delayed Processing
When intake QC is enforced:
- Cases with complete information proceed immediately
- Cases with missing data are paused until clarification is provided
If information cannot be provided promptly, cases are typically deferred to the next processing cycle.
Impact on Workflow Efficiency
While this approach may delay individual cases, it prevents:
- Interrupted design workflows
- Mid-process communication delays
- Redesign and remakes
From a system perspective, enforcing intake QC reduces total turnaround time across all cases.
The Cost of Skipping Intake Quality Control
When dental case intake quality control is not applied consistently, errors propagate through the workflow.
Design-Level Consequences
- Incorrect margin interpretation
- Unstable occlusion due to incomplete bite data
- Inconsistent anatomical design
Production-Level Consequences
- Poor fit requiring adjustment
- Material waste due to remakes
- Delays in delivery schedules
Operational Consequences
- Increased communication between lab and clinic
- Unpredictable turnaround times
- Reduced throughput capacity
These issues are often more costly to resolve than the time saved by skipping intake QC.
Intake QC as a Bottleneck Prevention Strategy
From a workflow perspective, intake QC functions as a bottleneck control mechanism.
Identifying Constraints Early
By validating cases before design:
- Errors are identified at the earliest possible stage
- Design teams are not interrupted mid-process
- Production schedules remain stable
Maintaining Continuous Workflow
When only validated cases enter the design queue:
- Designers can work without interruption
- Case flow becomes more predictable
- Resource allocation is more efficient
This transforms the workflow from reactive to controlled.
Interaction Between Intake QC and Turnaround Time
Turnaround time is often misunderstood as a measure of speed. In practice, it is a measure of consistency.
Structured Turnaround Logic
In disciplined workflows:
- Design timelines begin only after intake validation
- Cases with complete information follow defined turnaround windows
- Complex cases are allocated appropriate time based on requirements
For example, design timelines may vary depending on case size and complexity, but only after the case is confirmed to be complete.
Avoiding Hidden Delays
Without intake QC, delays occur later in the process:
- Waiting for missing information during design
- Reworking incomplete designs
- Reproducing failed cases
These delays are less visible but more disruptive.
Case Communication as Part of Intake Quality Control
Intake QC is closely tied to communication between clinics and laboratories.
Structured Communication Requirements
Effective intake processes define:
- Required scan sets
- Mandatory prescription fields
- Acceptable file formats
- Response expectations for missing data
This reduces ambiguity and ensures that both parties operate within the same framework.
Feedback Loops
When issues are identified:
- Clear feedback is provided to the clinic
- Specific deficiencies are documented
- Resubmission requirements are defined
Over time, this improves submission quality and reduces intake errors.
Managing Variability in Case Submissions
Not all cases are submitted with the same level of completeness or quality. Variability is inevitable due to differences in:
- Scanner systems
- Operator technique
- Clinical conditions
Standardization Through Intake QC
A structured dental case intake quality control process mitigates this variability by:
- Applying consistent validation criteria
- Rejecting or pausing incomplete cases
- Ensuring that only standardized inputs enter the workflow
This creates a stable foundation for design and production.
Prioritization and Case Segmentation
In high-volume environments, not all cases require the same level of urgency.
Role of Intake QC in Prioritization
During intake, cases can be categorized based on:
- Urgency
- Complexity
- Completeness of data
This allows laboratories to:
- Prioritize critical cases
- Allocate resources efficiently
- Maintain balance between speed and accuracy
Without intake QC, prioritization becomes reactive rather than planned.
Integration with Digital Case Management Systems
Modern workflows often incorporate digital tools for case tracking and management.
Benefits of Structured Case Management
- Centralized tracking of case status
- Visibility into intake validation results
- Coordination between design and production stages
Some systems provide shared dashboards or tracking links, enabling both laboratory and clinic to monitor case progress.
Impact on Workflow Transparency
This integration improves:
- Communication efficiency
- Accountability
- Predictability of delivery timelines
Two Approaches to Intake Handling
Different laboratories approach intake in different ways.
Approach 1: Immediate Processing
- Cases are accepted and sent directly to design
- Minimal validation at intake
- Issues addressed during or after design
Approach 2: Controlled Intake QC
- Cases are validated before entering the design queue
- Incomplete cases are paused
- Only standardized inputs proceed
The second approach leads to greater overall efficiency, despite appearing slower at the initial stage.
Limitations and Practical Considerations
While intake QC improves workflow stability, it requires:
- Clearly defined submission guidelines
- Consistent enforcement of validation criteria
- Efficient communication channels
Without these elements, intake QC may become a bottleneck rather than a control mechanism.
However, when implemented correctly, it functions as a filter that stabilizes the entire workflow.
Conclusion: Intake QC as the Foundation of Predictable Workflows
In digital dental workflows, dental case intake quality control is the foundation upon which all subsequent stages depend.
By ensuring that only complete, consistent, and compatible data enters the design process, intake QC reduces variability, prevents downstream errors, and supports predictable turnaround times.
For laboratories and clinics aiming to optimize efficiency and reduce rework, the focus should not begin at design or production, but at intake—where workflow stability is first established.
Occlusion is one of the most sensitive variables in crown and bridge restorations. In digital workflows, where design is executed through CAD systems and transferred directly to manufacturing, occlusal accuracy is determined not only by clinical intent but by how effectively that intent is translated into digital data and controlled within the design environment.
Occlusal design dental CAD is not a single step within the workflow. It is a layered process involving scan accuracy, articulation logic, design parameters, and manufacturing constraints. From a laboratory perspective, inconsistencies in occlusion are a primary source of chairside adjustments, remakes, and workflow inefficiency.
This article examines occlusal design from a lab-driven perspective, focusing on how digital workflows manage occlusion and where common breakdowns occur.
In analog workflows, technicians could adjust occlusion manually based on physical models and articulators. In digital workflows, occlusion is entirely dependent on the accuracy of the input data and the parameters defined within the CAD system.
The reliability of occlusal design dental CAD depends on:
If any of these inputs are compromised, occlusal relationships must be approximated during design, increasing variability in the final restoration.
Among all input factors, bite registration plays the most critical role in occlusal design.
Common issues include:
These issues directly affect how contact points are established in CAD.
When bite data is unreliable, designers must decide whether to:
Both approaches introduce risk. Reduced contacts may compromise function, while estimated contacts may require chairside adjustment.
Digital workflows primarily operate on static occlusion models. However, clinical function involves dynamic movement.
Most CAD systems define occlusion based on:
These parameters provide a controlled environment for design but do not fully replicate functional movements.
While some systems offer virtual articulation, they are limited by:
As a result, occlusal design dental CAD must balance static accuracy with practical considerations for functional adaptation.
Occlusal design is not only about establishing contact but also about controlling how contact is distributed.
Proper distribution ensures that:
In digital workflows, this is managed through contact mapping tools that visualize occlusal pressure zones.
CAD systems allow designers to define:
These settings influence how the restoration interacts with opposing dentition.
Achieving the correct balance depends on both input accuracy and design control.
Occlusal design must account for the material used in the restoration. Different materials respond differently to occlusal forces.
In occlusal design dental CAD, material selection influences:
Ignoring these factors can lead to material failure or functional issues.
Occlusal clearance refers to the space between the restoration and the opposing dentition.
Adequate clearance ensures:
Designers define clearance values within the CAD system. These values must account for:
Incorrect clearance settings can result in either tight occlusion or lack of contact.
Occlusal design must be translated accurately into physical form during production.
Modern manufacturing systems can reproduce design geometry with high precision. However, they do not correct design errors.
If occlusal relationships are incorrect in CAD:
Consistent occlusal design dental CAD ensures that:
Quality control for occlusion is integrated into multiple stages of the workflow.
This multi-layered approach reduces the likelihood of occlusal discrepancies reaching the clinical stage.
Occlusal design is highly dependent on clinical input. Without clear communication, even accurate data may be misinterpreted.
When communication is incomplete:
Structured communication protocols help align clinical intent with laboratory execution.
Variability in occlusion arises from multiple sources:
To manage this variability, laboratories implement:
These strategies help maintain stability in occlusal design dental CAD across different cases.
In high-volume environments, there is often a trade-off between speed and precision.
From a workflow perspective, prioritizing occlusal precision improves overall efficiency by reducing rework and adjustment time.
Despite advancements in CAD technology, certain limitations remain:
These limitations require designers to apply judgment and experience when interpreting digital data.
In digital crown and bridge workflows, occlusal design dental CAD is a controlled variable that must be managed across multiple stages.
From bite registration and contact distribution to material considerations and manufacturing alignment, each element contributes to the final outcome. While CAD systems provide tools for precision, the reliability of occlusal design depends on the quality of input data, the consistency of design protocols, and the integration of workflow stages.
For laboratories and clinics aiming to reduce adjustments and improve predictability, occlusion must be treated as a system-level consideration rather than an isolated design task.
Occlusal design dental CAD is not a single step within the workflow. It is a layered process involving scan accuracy, articulation logic, design parameters, and manufacturing constraints. From a laboratory perspective, inconsistencies in occlusion are a primary source of chairside adjustments, remakes, and workflow inefficiency.
This article examines occlusal design from a lab-driven perspective, focusing on how digital workflows manage occlusion and where common breakdowns occur.
Occlusion as a Data-Dependent Variable in Digital Workflows
In analog workflows, technicians could adjust occlusion manually based on physical models and articulators. In digital workflows, occlusion is entirely dependent on the accuracy of the input data and the parameters defined within the CAD system.
The reliability of occlusal design dental CAD depends on:
- Accuracy of bite registration
- Alignment of upper and lower arches
- Completeness of occlusal surface data
- Stability of articulation within the software
If any of these inputs are compromised, occlusal relationships must be approximated during design, increasing variability in the final restoration.
Bite Registration: The Primary Determinant of Occlusal Accuracy
Among all input factors, bite registration plays the most critical role in occlusal design.
Digital Bite Alignment Challenges
Common issues include:
- Inconsistent bite capture leading to unstable occlusion
- Misalignment between arches due to stitching errors
- Partial bite scans that do not represent full occlusal contact
These issues directly affect how contact points are established in CAD.
Impact on Design Decisions
When bite data is unreliable, designers must decide whether to:
- Reduce occlusal contacts to avoid high points
- Maintain estimated contacts based on anatomical assumptions
Both approaches introduce risk. Reduced contacts may compromise function, while estimated contacts may require chairside adjustment.
Static vs. Functional Occlusion in CAD Environments
Digital workflows primarily operate on static occlusion models. However, clinical function involves dynamic movement.
Static Occlusion in CAD
Most CAD systems define occlusion based on:
- Maximum intercuspation position (MIP)
- Contact intensity mapping
- Interocclusal clearance settings
These parameters provide a controlled environment for design but do not fully replicate functional movements.
Limitations in Functional Simulation
While some systems offer virtual articulation, they are limited by:
- Accuracy of input data
- Simplified movement models
- Lack of patient-specific functional dynamics
As a result, occlusal design dental CAD must balance static accuracy with practical considerations for functional adaptation.
Contact Design: Distribution, Intensity, and Control
Occlusal design is not only about establishing contact but also about controlling how contact is distributed.
Contact Distribution
Proper distribution ensures that:
- Forces are evenly shared across the restoration
- No single contact point bears excessive load
In digital workflows, this is managed through contact mapping tools that visualize occlusal pressure zones.
Contact Intensity
CAD systems allow designers to define:
- Light contact
- Normal contact
- Heavy contact
These settings influence how the restoration interacts with opposing dentition.
Risk of Over- or Under-Contact
- Excessive contact leads to high points and adjustment requirements
- Insufficient contact leads to lack of function and instability
Achieving the correct balance depends on both input accuracy and design control.
Material Considerations in Occlusal Design
Occlusal design must account for the material used in the restoration. Different materials respond differently to occlusal forces.
Material-Specific Constraints
- Zirconia requires controlled contact to avoid excessive stress
- Layered restorations may require reduced occlusal load
- Monolithic restorations allow for more direct force distribution
Design Implications
In occlusal design dental CAD, material selection influences:
- Contact intensity settings
- Occlusal anatomy design
- Thickness and structural support
Ignoring these factors can lead to material failure or functional issues.
Occlusal Clearance and Its Role in Manufacturing
Occlusal clearance refers to the space between the restoration and the opposing dentition.
Importance of Clearance Control
Adequate clearance ensures:
- Proper seating of the restoration
- Avoidance of premature contact
- Compatibility with manufacturing tolerances
CAD Parameter Management
Designers define clearance values within the CAD system. These values must account for:
- Milling or printing tolerances
- Material shrinkage or expansion
- Cement space interaction
Incorrect clearance settings can result in either tight occlusion or lack of contact.
The Transition from Design to Manufacturing
Occlusal design must be translated accurately into physical form during production.
Manufacturing Precision vs. Design Accuracy
Modern manufacturing systems can reproduce design geometry with high precision. However, they do not correct design errors.
If occlusal relationships are incorrect in CAD:
- Milling will reproduce those inaccuracies
- Post-processing cannot fully correct them
Consistency Across Production
Consistent occlusal design dental CAD ensures that:
- Restorations fit within expected occlusal parameters
- Adjustments are minimized
- Workflow efficiency is maintained
Quality Control in Occlusal Design
Quality control for occlusion is integrated into multiple stages of the workflow.
Design-Level QC
- Verification of contact points
- Review of occlusal clearance
- Assessment of articulation alignment
Pre-Production QC
- Simulation of occlusal interaction
- Validation against design parameters
Post-Production QC
- Physical or digital verification of contact areas
This multi-layered approach reduces the likelihood of occlusal discrepancies reaching the clinical stage.
Communication Between Clinic and Laboratory
Occlusal design is highly dependent on clinical input. Without clear communication, even accurate data may be misinterpreted.
Required Clinical Information
- Occlusal scheme preferences
- Functional considerations
- Any specific adjustments required
Impact on Workflow
When communication is incomplete:
- Designers must rely on default settings
- Variability increases
- Adjustment rates rise
Structured communication protocols help align clinical intent with laboratory execution.
Managing Variability in Occlusal Design
Variability in occlusion arises from multiple sources:
- Differences in scanning technique
- Variations in bite registration
- Case-specific anatomical factors
Workflow Strategies
To manage this variability, laboratories implement:
- Standardized design parameters
- Defined occlusal protocols
- Consistent QC procedures
These strategies help maintain stability in occlusal design dental CAD across different cases.
Balancing Efficiency and Occlusal Precision
In high-volume environments, there is often a trade-off between speed and precision.
Efficiency-Focused Approach
- Faster design with minimal adjustments
- Higher risk of occlusal discrepancies
- Increased chairside correction
Precision-Focused Approach
- Detailed occlusal analysis during design
- Reduced need for clinical adjustment
- More predictable outcomes
From a workflow perspective, prioritizing occlusal precision improves overall efficiency by reducing rework and adjustment time.
Limitations of Digital Occlusal Design
Despite advancements in CAD technology, certain limitations remain:
- Dependence on input data quality
- Simplified articulation models
- Limited representation of dynamic function
These limitations require designers to apply judgment and experience when interpreting digital data.
Conclusion: Occlusion as a Controlled Variable in Digital Design
In digital crown and bridge workflows, occlusal design dental CAD is a controlled variable that must be managed across multiple stages.
From bite registration and contact distribution to material considerations and manufacturing alignment, each element contributes to the final outcome. While CAD systems provide tools for precision, the reliability of occlusal design depends on the quality of input data, the consistency of design protocols, and the integration of workflow stages.
For laboratories and clinics aiming to reduce adjustments and improve predictability, occlusion must be treated as a system-level consideration rather than an isolated design task.

In digital crown and bridge workflows, most downstream issues—misfit, open margins, occlusal discrepancies, and remakes—can often be traced back to a single upstream variable: margin definition. While CAD systems and manufacturing technologies continue to improve in precision, they remain dependent on the accuracy of the preparation margin captured during scanning.
Crown margin accuracy is not simply a technical detail within the design phase. It is a controlling factor that determines how reliably a restoration seats, how much adjustment is required chairside, and how often cases must be remade. From a laboratory perspective, margin clarity directly influences both workflow efficiency and production predictability.
This article examines how margin quality affects crown fit, why unclear margins increase remake rates, and how structured workflows mitigate these risks.
In CAD-based workflows, the margin line defines the boundary between the prepared tooth and the restoration. It serves as the primary reference for:
When crown margin accuracy is high, the design process can proceed with confidence. The CAD system can:
However, when margin clarity is compromised, the design process becomes interpretive rather than deterministic. The designer must approximate the margin location, introducing variability into the final result.
Crown fit is directly tied to how precisely the margin is defined in the digital model.
When margins are:
the resulting crown is more likely to:
This leads to consistent clinical outcomes and reduced chairside time.
When margins are:
the resulting crown may exhibit:
These issues are not always correctable through minor adjustments and often lead to compromised results or remakes.
From a laboratory operations perspective, remake rates are a critical indicator of workflow efficiency. Among the various causes of remakes, margin-related issues are consistently among the most significant.
Each of these issues originates from insufficient crown margin accuracy at the input stage.
Remakes introduce multiple layers of inefficiency:
Reducing remake rates therefore depends heavily on improving margin clarity at the beginning of the workflow.
A common assumption is that advanced CAD software can compensate for unclear margins. In practice, this is not the case.
CAD systems rely on geometric contrast to identify margin lines. When this contrast is insufficient:
Even with manual intervention, the absence of clear data limits the accuracy of the final design.
When crown margin accuracy is compromised, designers must choose between:
Neither option guarantees optimal fit, and both increase the likelihood of adjustment or remake.
Margin definition does not only affect the external boundary of the crown. It also determines how internal parameters are applied.
Cement space is typically defined relative to the margin line. If the margin is unclear:
Accurate margins allow for:
Poor margin data disrupts these relationships, leading to unpredictable internal fit.
Margin clarity is influenced by multiple aspects of scan quality. These factors must be considered collectively to ensure reliable crown margin accuracy.
Margins located near or below the gingival margin are particularly sensitive to:
If soft tissue obscures the margin, scan data becomes incomplete.
Scanner resolution affects the ability to capture fine margin details. Low-resolution scans may:
Inconsistent scanning paths can lead to:
These issues are often subtle but significantly affect design accuracy.
Given the importance of margin clarity, structured laboratories incorporate margin validation into the intake process.
Before design begins, cases are evaluated for:
If margins are insufficiently defined, cases may be paused for clarification or rescanning.
While this step may delay individual cases, it prevents:
From a system perspective, early validation improves overall efficiency.
Margin accuracy is not solely a technical issue; it is also a communication issue.
In addition to scan data, laboratories rely on:
When communication is incomplete, even high-quality scans may be interpreted incorrectly.
Structured workflows include feedback mechanisms:
Over time, this reduces variability in crown margin accuracy across cases.
Once design is completed, production systems replicate the digital model with high precision. However, they cannot correct margin inaccuracies.
Milling and printing systems:
Therefore, production consistency is directly tied to margin accuracy in the design phase.
Inaccurate margins affect:
These factors extend beyond workflow efficiency into clinical performance.
In high-volume environments, there is often pressure to accelerate workflows. However, margin accuracy requires careful data capture and validation.
From a workflow perspective, prioritizing crown margin accuracy leads to greater efficiency over the full production cycle.
Variability in margin clarity is inevitable due to differences in:
Structured workflows manage this variability through:
By controlling how margin data is evaluated and processed, laboratories can reduce its impact on final outcomes.
In digital crown workflows, crown margin accuracy is a primary control variable that determines both fit and remake rates.
Clear, well-defined margins enable precise CAD design, consistent manufacturing, and predictable clinical outcomes. Conversely, unclear margins introduce variability at every stage, leading to increased adjustments and higher remake rates.
For laboratories and clinics aiming to optimize workflow efficiency and restoration quality, margin clarity should be treated not as a secondary detail, but as a foundational requirement.
Crown margin accuracy is not simply a technical detail within the design phase. It is a controlling factor that determines how reliably a restoration seats, how much adjustment is required chairside, and how often cases must be remade. From a laboratory perspective, margin clarity directly influences both workflow efficiency and production predictability.
This article examines how margin quality affects crown fit, why unclear margins increase remake rates, and how structured workflows mitigate these risks.
Margin Definition as the Starting Point of Crown Design
In CAD-based workflows, the margin line defines the boundary between the prepared tooth and the restoration. It serves as the primary reference for:
- Restoration seating
- Internal fit and cement space
- External contour emergence
- Margin adaptation
When crown margin accuracy is high, the design process can proceed with confidence. The CAD system can:
- Detect the margin automatically or with minimal manual refinement
- Generate consistent offsets for cement space
- Maintain uniform adaptation along the entire margin line
However, when margin clarity is compromised, the design process becomes interpretive rather than deterministic. The designer must approximate the margin location, introducing variability into the final result.
How Margin Clarity Influences Crown Fit
Crown fit is directly tied to how precisely the margin is defined in the digital model.
Clear Margins and Predictable Seating
When margins are:
- Sharp and continuous
- Free from noise or distortion
- Fully captured circumferentially
the resulting crown is more likely to:
- Seat fully without resistance
- Maintain uniform internal spacing
- Require minimal adjustment
This leads to consistent clinical outcomes and reduced chairside time.
Unclear Margins and Fit Variability
When margins are:
- Blurred by soft tissue interference
- Interrupted by missing scan data
- Distorted by mesh irregularities
the resulting crown may exhibit:
- Tight or incomplete seating
- Open or overextended margins
- Uneven internal contact
These issues are not always correctable through minor adjustments and often lead to compromised results or remakes.
The Relationship Between Margin Accuracy and Remake Rates
From a laboratory operations perspective, remake rates are a critical indicator of workflow efficiency. Among the various causes of remakes, margin-related issues are consistently among the most significant.
Common Margin-Related Causes of Remakes
- Incorrect margin placement during design
- Incomplete margin capture leading to open edges
- Overcompensation by designers resulting in overextended margins
- Misinterpretation of unclear margin boundaries
Each of these issues originates from insufficient crown margin accuracy at the input stage.
Workflow Impact of Remakes
Remakes introduce multiple layers of inefficiency:
- Additional design time
- Reproduction and material usage
- Communication and coordination delays
- Disruption of production scheduling
Reducing remake rates therefore depends heavily on improving margin clarity at the beginning of the workflow.
Why CAD Systems Cannot Compensate for Poor Margin Data
A common assumption is that advanced CAD software can compensate for unclear margins. In practice, this is not the case.
Limitations of Automated Margin Detection
CAD systems rely on geometric contrast to identify margin lines. When this contrast is insufficient:
- Automatic detection becomes unreliable
- Manual marking becomes necessary
- Variability between designers increases
Even with manual intervention, the absence of clear data limits the accuracy of the final design.
Design Constraints Imposed by Input Quality
When crown margin accuracy is compromised, designers must choose between:
- Conservative margin placement (risking open margins)
- Aggressive margin placement (risking overextension)
Neither option guarantees optimal fit, and both increase the likelihood of adjustment or remake.
Margin Clarity and Its Effect on Cement Space and Internal Fit
Margin definition does not only affect the external boundary of the crown. It also determines how internal parameters are applied.
Cement Space Distribution
Cement space is typically defined relative to the margin line. If the margin is unclear:
- Cement space may be inconsistent
- Internal pressure points may develop
- Seating may be incomplete
Internal Adaptation
Accurate margins allow for:
- Uniform internal spacing
- Controlled retention and resistance form
- Predictable seating behavior
Poor margin data disrupts these relationships, leading to unpredictable internal fit.
Scan Quality Factors That Affect Margin Accuracy
Margin clarity is influenced by multiple aspects of scan quality. These factors must be considered collectively to ensure reliable crown margin accuracy.
Soft Tissue Management
Margins located near or below the gingival margin are particularly sensitive to:
- Tissue interference
- Moisture contamination
- Limited scanner access
If soft tissue obscures the margin, scan data becomes incomplete.
Resolution and Detail Capture
Scanner resolution affects the ability to capture fine margin details. Low-resolution scans may:
- Smooth out sharp edges
- Blur margin transitions
- Reduce geometric contrast
Scan Path and Technique
Inconsistent scanning paths can lead to:
- Stitching errors
- Distorted geometry
- Incomplete margin capture
These issues are often subtle but significantly affect design accuracy.
Laboratory Intake and Margin Validation
Given the importance of margin clarity, structured laboratories incorporate margin validation into the intake process.
Intake-Level Margin Assessment
Before design begins, cases are evaluated for:
- Margin continuity
- Clarity and contrast
- Completeness around the entire preparation
If margins are insufficiently defined, cases may be paused for clarification or rescanning.
Impact on Workflow Efficiency
While this step may delay individual cases, it prevents:
- Incorrect design execution
- Downstream production errors
- Increased remake rates
From a system perspective, early validation improves overall efficiency.
Communication Between Clinic and Laboratory
Margin accuracy is not solely a technical issue; it is also a communication issue.
Importance of Clear Case Instructions
In addition to scan data, laboratories rely on:
- Margin location confirmation
- Preparation type and expectations
- Any specific design considerations
When communication is incomplete, even high-quality scans may be interpreted incorrectly.
Feedback Loops for Margin Improvement
Structured workflows include feedback mechanisms:
- Identification of margin issues
- Documentation of deficiencies
- Guidance for improved scanning
Over time, this reduces variability in crown margin accuracy across cases.
Margin Accuracy and Production Consistency
Once design is completed, production systems replicate the digital model with high precision. However, they cannot correct margin inaccuracies.
Manufacturing Dependence on Design Accuracy
Milling and printing systems:
- Follow the defined margin line precisely
- Maintain the geometry provided by CAD
- Reproduce both accurate and inaccurate designs equally
Therefore, production consistency is directly tied to margin accuracy in the design phase.
Implications for Fit and Longevity
Inaccurate margins affect:
- Crown seating
- Cement integrity
- Long-term stability of the restoration
These factors extend beyond workflow efficiency into clinical performance.
Balancing Speed and Margin Quality
In high-volume environments, there is often pressure to accelerate workflows. However, margin accuracy requires careful data capture and validation.
Speed-Oriented Approach
- Faster scanning with minimal verification
- Increased risk of unclear margins
- Higher likelihood of adjustment and remake
Accuracy-Oriented Approach
- Additional time spent ensuring margin clarity
- Reduced need for redesign or correction
- More predictable outcomes
From a workflow perspective, prioritizing crown margin accuracy leads to greater efficiency over the full production cycle.
Managing Variability in Margin Quality
Variability in margin clarity is inevitable due to differences in:
- Clinical conditions
- Scanner systems
- Operator technique
Structured workflows manage this variability through:
- Standardized intake criteria
- Consistent design protocols
- Defined communication channels
By controlling how margin data is evaluated and processed, laboratories can reduce its impact on final outcomes.
Conclusion: Margin Clarity as a Primary Control Variable
In digital crown workflows, crown margin accuracy is a primary control variable that determines both fit and remake rates.
Clear, well-defined margins enable precise CAD design, consistent manufacturing, and predictable clinical outcomes. Conversely, unclear margins introduce variability at every stage, leading to increased adjustments and higher remake rates.
For laboratories and clinics aiming to optimize workflow efficiency and restoration quality, margin clarity should be treated not as a secondary detail, but as a foundational requirement.

In digital dentistry, accuracy is often attributed to software capability or manufacturing precision. However, in practical laboratory workflows, the limiting factor is frequently upstream: the quality of the submitted digital files. Regardless of how advanced the CAD system or production equipment may be, the output can only be as accurate as the data it is built upon.
Dental CAD file quality directly influences how reliably a restoration can be designed, validated, and manufactured. It affects not only the geometry of the final restoration but also the efficiency of the entire workflow—from intake and design to production and delivery.
This article examines how file quality—particularly STL and intraoral scan data—determines CAD design accuracy, and how its impact propagates through each stage of the dental workflow.
CAD systems operate on geometric input. Unlike analog workflows where technicians can compensate visually or manually, digital workflows rely strictly on the data provided.
When dental CAD file quality is compromised, the system does not “interpret” missing or unclear information. Instead, it generates a design based on incomplete or distorted geometry. This leads to:
These issues are not always immediately visible during design but become evident during try-in or after fabrication.
In this sense, CAD design accuracy is not created during the design phase—it is constrained by the quality of the input data.
Most digital dental workflows rely on STL or similar mesh-based file formats to represent 3D geometry. These files are generated from intraoral scanners or laboratory scanners and form the foundation for all subsequent processes.
Key characteristics of high-quality scan data include:
When these conditions are met, CAD systems can reliably identify reference points and generate consistent designs.
However, when dental CAD file quality is compromised, the system must rely on approximations, increasing variability in the output.
Among all aspects of a scan, margin clarity is one of the most critical for CAD design.
If margins are:
then the design software cannot accurately define the preparation boundary.
This leads to:
From a laboratory perspective, unclear margins are one of the most common causes of redesign requests or case delays.
When margin clarity is insufficient, the workflow is interrupted:
Therefore, margin quality is not only a technical factor but also a workflow determinant.
Occlusal accuracy depends on how well the relationship between upper and lower arches is captured.
When dental CAD file quality is insufficient in this area, designers must either:
Inaccurate occlusion affects:
From a workflow standpoint, it introduces variability that cannot be fully corrected during manufacturing.
Beyond visible features such as margins and occlusion, the internal structure of the scan file—its mesh integrity—plays a critical role.
These issues may not always be obvious visually but can affect how CAD software processes the file.
Poor mesh integrity can lead to:
In some cases, files must be repaired or reprocessed before design can begin, adding time and complexity to the workflow.
Consistency across cases is a key requirement in laboratory workflows. However, variability in dental CAD file quality introduces inconsistency at the earliest stage.
Even when using standardized design protocols:
This creates uneven workload distribution within design teams and reduces overall efficiency.
When file quality varies significantly between cases:
From a system perspective, maintaining consistent input quality is essential for achieving consistent output.
While CAD design defines the geometry of a restoration, manufacturing translates that geometry into a physical object.
Production technologies such as milling and 3D printing operate with high precision. However, they cannot compensate for:
If the design is based on poor-quality input, manufacturing will reproduce those inaccuracies with high fidelity.
High dental CAD file quality ensures that:
Without this alignment, even advanced manufacturing systems cannot achieve predictable results.
Given the impact of file quality, structured workflows incorporate quality control at the intake stage.
Cases that do not meet minimum quality thresholds are typically paused until corrections are made.
While intake QC may delay individual cases, it prevents:
From a broader perspective, it improves overall workflow efficiency and predictability.
File quality is not solely a technical issue; it is also a communication issue between clinics and laboratories.
When file quality issues are identified:
This creates a feedback loop that gradually improves submission quality over time.
Consistent communication regarding dental CAD file quality leads to:
Over time, this stabilizes the entire digital workflow.
In practice, there is often pressure to prioritize speed over data quality. However, these two factors are interdependent.
From a workflow perspective, prioritizing dental CAD file quality leads to greater efficiency over the full case lifecycle, even if initial submission takes slightly longer.
While high file quality is essential, it is influenced by factors beyond the laboratory’s control:
Outsourcing partners must account for these variables by:
However, the fundamental principle remains: design accuracy cannot exceed input accuracy.
In digital dental workflows, dental CAD file quality is the primary determinant of design accuracy and overall workflow efficiency.
From margin definition and occlusion to manufacturing consistency, every stage depends on the integrity of the input data. While advanced CAD systems and production technologies enhance precision, they cannot compensate for deficiencies in the original scan.
For laboratories and clinics aiming to achieve predictable outcomes, improving file quality is not a secondary consideration—it is the foundation upon which the entire workflow is built.
Dental CAD file quality directly influences how reliably a restoration can be designed, validated, and manufactured. It affects not only the geometry of the final restoration but also the efficiency of the entire workflow—from intake and design to production and delivery.
This article examines how file quality—particularly STL and intraoral scan data—determines CAD design accuracy, and how its impact propagates through each stage of the dental workflow.
CAD Design Accuracy Begins at the Data Level
CAD systems operate on geometric input. Unlike analog workflows where technicians can compensate visually or manually, digital workflows rely strictly on the data provided.
When dental CAD file quality is compromised, the system does not “interpret” missing or unclear information. Instead, it generates a design based on incomplete or distorted geometry. This leads to:
- Inaccurate margin detection
- Improper occlusal relationships
- Misaligned contacts or emergence profiles
These issues are not always immediately visible during design but become evident during try-in or after fabrication.
In this sense, CAD design accuracy is not created during the design phase—it is constrained by the quality of the input data.
Understanding the Role of STL and Scan Data in Design
Most digital dental workflows rely on STL or similar mesh-based file formats to represent 3D geometry. These files are generated from intraoral scanners or laboratory scanners and form the foundation for all subsequent processes.
Key characteristics of high-quality scan data include:
- Complete surface capture without missing areas
- Clear margin definition with minimal noise
- Accurate spatial relationships between arches
- Stable mesh integrity without distortions or holes
When these conditions are met, CAD systems can reliably identify reference points and generate consistent designs.
However, when dental CAD file quality is compromised, the system must rely on approximations, increasing variability in the output.
Margin Definition: The Most Sensitive Indicator of File Quality
Among all aspects of a scan, margin clarity is one of the most critical for CAD design.
Impact of Poor Margin Capture
If margins are:
- Blurred due to soft tissue interference
- Incomplete due to scanning limitations
- Distorted due to mesh irregularities
then the design software cannot accurately define the preparation boundary.
This leads to:
- Overextended or underextended margins
- Poor seating of restorations
- Increased need for chairside adjustment
From a laboratory perspective, unclear margins are one of the most common causes of redesign requests or case delays.
Relationship to Workflow Efficiency
When margin clarity is insufficient, the workflow is interrupted:
- Additional communication is required to clarify the margin
- Cases may be paused pending updated scans
- Design timelines become unpredictable
Therefore, margin quality is not only a technical factor but also a workflow determinant.
Occlusion and Bite Registration Accuracy
Occlusal accuracy depends on how well the relationship between upper and lower arches is captured.
Common Issues with Low-Quality Bite Data
- Inconsistent bite registration leading to incorrect articulation
- Misaligned arch positioning due to scanning errors
- Incomplete occlusal surfaces affecting contact design
When dental CAD file quality is insufficient in this area, designers must either:
- Adjust occlusion based on assumptions
- Request additional data
- Accept a higher risk of occlusal adjustment post-production
Downstream Effects
Inaccurate occlusion affects:
- Functional performance of restorations
- Patient comfort
- Time required for clinical adjustments
From a workflow standpoint, it introduces variability that cannot be fully corrected during manufacturing.
Mesh Integrity and Its Influence on Design Stability
Beyond visible features such as margins and occlusion, the internal structure of the scan file—its mesh integrity—plays a critical role.
Common Mesh Issues
- Holes or missing polygons
- Overlapping or intersecting surfaces
- Noise artifacts from scanning errors
- Uneven mesh density
These issues may not always be obvious visually but can affect how CAD software processes the file.
Impact on CAD Operations
Poor mesh integrity can lead to:
- Errors in automated margin detection
- Instability during Boolean operations
- Inconsistent thickness calculations
In some cases, files must be repaired or reprocessed before design can begin, adding time and complexity to the workflow.
File Quality and Its Effect on Design Consistency
Consistency across cases is a key requirement in laboratory workflows. However, variability in dental CAD file quality introduces inconsistency at the earliest stage.
Variability in Input Leads to Variability in Output
Even when using standardized design protocols:
- High-quality files produce predictable results
- Low-quality files require manual intervention or adjustments
This creates uneven workload distribution within design teams and reduces overall efficiency.
Standardization Challenges
When file quality varies significantly between cases:
- Design timelines become inconsistent
- Quality control becomes more complex
- Remake rates may increase
From a system perspective, maintaining consistent input quality is essential for achieving consistent output.
The Role of File Quality in Manufacturing Accuracy
While CAD design defines the geometry of a restoration, manufacturing translates that geometry into a physical object.
Limitations of Manufacturing Compensation
Production technologies such as milling and 3D printing operate with high precision. However, they cannot compensate for:
- Incorrect margins
- Misaligned occlusion
- Distorted geometry
If the design is based on poor-quality input, manufacturing will reproduce those inaccuracies with high fidelity.
Alignment Between Design and Production
High dental CAD file quality ensures that:
- Design intent is accurately translated into production
- Material thickness and structural integrity are maintained
- Fit and function are consistent with design parameters
Without this alignment, even advanced manufacturing systems cannot achieve predictable results.
Intake Quality Control as a Workflow Necessity
Given the impact of file quality, structured workflows incorporate quality control at the intake stage.
Key Elements of Intake QC
- Verification of required scan sets (preparation, antagonist, bite)
- Assessment of margin clarity and completeness
- Evaluation of mesh integrity
- Identification of missing or inconsistent data
Cases that do not meet minimum quality thresholds are typically paused until corrections are made.
Workflow Implications
While intake QC may delay individual cases, it prevents:
- Design errors
- Production failures
- Remakes and rework
From a broader perspective, it improves overall workflow efficiency and predictability.
Communication and File Quality Feedback Loops
File quality is not solely a technical issue; it is also a communication issue between clinics and laboratories.
Importance of Structured Feedback
When file quality issues are identified:
- Clear feedback must be provided to the submitting clinic
- Specific deficiencies should be documented
- Guidance on resubmission should be defined
This creates a feedback loop that gradually improves submission quality over time.
Long-Term Workflow Benefits
Consistent communication regarding dental CAD file quality leads to:
- Fewer rejected cases
- Reduced turnaround variability
- Improved collaboration between clinic and lab
Over time, this stabilizes the entire digital workflow.
Balancing Speed and Data Quality
In practice, there is often pressure to prioritize speed over data quality. However, these two factors are interdependent.
Perspective 1: Speed-Driven Submission
- Faster case submission with minimal verification
- Higher likelihood of incomplete or low-quality data
- Increased downstream delays
Perspective 2: Quality-Driven Submission
- Additional time spent ensuring scan completeness and clarity
- Reduced need for redesign or communication
- More predictable overall turnaround
From a workflow perspective, prioritizing dental CAD file quality leads to greater efficiency over the full case lifecycle, even if initial submission takes slightly longer.
Limitations and Practical Considerations
While high file quality is essential, it is influenced by factors beyond the laboratory’s control:
- Scanner capabilities and calibration
- Operator technique
- Clinical environment (e.g., moisture control, access)
Outsourcing partners must account for these variables by:
- Defining minimum quality requirements
- Providing clear submission guidelines
- Maintaining flexibility in handling borderline cases
However, the fundamental principle remains: design accuracy cannot exceed input accuracy.
Conclusion: File Quality as the First Determinant of Accuracy
In digital dental workflows, dental CAD file quality is the primary determinant of design accuracy and overall workflow efficiency.
From margin definition and occlusion to manufacturing consistency, every stage depends on the integrity of the input data. While advanced CAD systems and production technologies enhance precision, they cannot compensate for deficiencies in the original scan.
For laboratories and clinics aiming to achieve predictable outcomes, improving file quality is not a secondary consideration—it is the foundation upon which the entire workflow is built.