Choosing a Dental Outsourcing partner is not only a purchasing decision. It is a workflow decision that affects case intake, design consistency, turnaround stability, manufacturing predictability, and remake risk across the entire restorative process. For dental labs, clinics, prosthodontists, and oral surgeons, the right partner should do more than accept files and return restorations. The partner should function as a dependable technical extension of the internal workflow.
That distinction matters because outsourcing can either reduce operational pressure or quietly increase it. A partner may appear capable based on service range alone, yet still create friction through inconsistent communication, weak file handling, unclear design standards, or unstable production output. On the other hand, a well-structured outsourcing workflow can improve consistency precisely because it introduces discipline where many internal systems become overloaded or variable.
For this reason, evaluating a Dental Outsourcing partner should not begin with broad claims. It should begin with practical questions. How does the partner review incoming files? How are design decisions controlled? How does the team manage implant-specific requirements? What happens when a case is incomplete? How predictable is the workflow across routine and complex cases? These are the questions that reveal whether the partner supports reliability or merely processes volume.
A common mistake is to judge a Dental Outsourcing partner mainly by the number of services listed. A broad menu may sound impressive: crown and bridge, implants, removable dentures, night guards, surgical guides, CAD design support, and other digital solutions. But service breadth alone does not prove operational reliability. A partner can offer many categories and still perform inconsistently if the underlying workflow lacks structure.
A more useful starting point is workflow discipline. A reliable partner should show clear case intake rules, defined review steps, organized communication channels, and technical standards that remain stable from one case to the next. This does not mean every case is treated identically. It means the process is coherent enough that the submitting team knows how cases will be handled and what information is required at each stage.
From one perspective, labs want flexibility. From another, they need predictability even more. The strongest Dental Outsourcing relationships usually combine both: flexibility in case handling, but structure in process. Without that structure, flexibility turns into improvisation, and improvisation is a poor foundation for consistency.
A reliable outsourcing partner does not treat every submitted case as immediately ready for production. The partner should first determine whether the file package is complete and usable. This is one of the clearest operational indicators of quality because weak intake review often leads to later delays, redesign, or remakes.
In a strong Dental Outsourcing workflow, the intake process should verify scan completeness, restoration type, bite relationships, relevant case notes, and any category-specific requirements such as implant system details or design references. If important information is missing, the partner should identify the issue early rather than designing around assumption.
This matters because a partner who begins work without validating the input may appear fast at first while actually creating hidden instability. A case that moves into CAD with incomplete data can return later with far greater disruption. By contrast, a partner who reviews before designing may appear slightly stricter at intake, but often delivers a more dependable workflow overall.
In practical terms, good intake review is a quality signal. It shows that the partner is protecting the case before value is added, not only inspecting it after risk has already entered the system.
Even highly skilled production teams become unreliable when communication is vague, delayed, or inconsistent. This is especially true in Dental Outsourcing, where the external team does not share the same room, case history, or informal discussions as the sending lab or clinic. If the workflow depends on unspoken assumptions, problems tend to surface later and at higher cost.
A dependable partner should communicate clearly at three stages: before design starts, during clarification if needed, and when the case moves into completion or release. That communication should be precise rather than overly broad. The point is not to generate more messages. The point is to reduce ambiguity.
For example, if scan quality is weak, the partner should specify what is missing. If an implant case lacks component clarity, the partner should identify that directly. If a complex case needs more review time, that should be visible early rather than discovered when the expected delivery point has already passed.
There are two different kinds of outsourcing communication. One is reactive and vague, usually appearing only when something has already gone wrong. The other is structured and early, helping the case stay stable before problems grow. A reliable Dental Outsourcing partner should operate in the second mode.
A partner may have capable technicians and advanced software, but reliability still depends on whether design decisions are applied consistently. Similar cases should not receive dramatically different occlusal logic, contact behavior, margin handling, connector planning, or emergence design simply because they were processed on different days or by different designers.
This is why a trustworthy Dental Outsourcing partner should demonstrate stable CAD standards. Crown and bridge cases should reflect repeatable logic in fit, contact, and occlusion. Bridge cases should be designed with consistent attention to connector behavior and insertion logic. Implant restorations should follow disciplined control around component compatibility, access positioning, and restorative space.
The real issue here is not artistic variation. It is technical repeatability. Labs do not gain reliability from stylistic fluctuation. They gain it from design consistency that supports predictable manufacturing and adjustment behavior.
From one angle, CAD design is a creative technical task. From another, it is also a system task. The best partner understands both. The team must be able to adapt to case-specific demands without abandoning core design discipline.
One of the most important differences between a useful partner and a weak one is manufacturing awareness. A file processor may produce a visually acceptable design. A real laboratory partner produces a design that is appropriate for how the case will actually be fabricated.
This matters because Dental Outsourcing does not end at the screen. Restorations move into milling, printing, sintering, finishing, assembly, and final inspection. If the design stage ignores manufacturing behavior, the case may look correct digitally while still performing poorly in production. Thickness management, connector structure, access positioning, internal fit logic, and post-processing feasibility all influence whether the restoration remains stable beyond the CAD phase.
A reliable partner therefore designs with production in mind. That is especially critical in implant work, long-span bridges, removable cases, and any workflow where small digital decisions can create large downstream consequences. The more complex the case, the more important this manufacturing awareness becomes.
A practical test is simple: does the partner seem to understand not just how to generate the file, but how that file will behave as a manufactured restoration? If the answer is unclear, the partnership may be technically shallow.
If there is one area where reliability is easiest to expose, it is implant prosthetics. Implant cases demand stricter control because they involve more than anatomy and occlusion. They depend on library verification, scan body interpretation, retention method, restorative space, component compatibility, and interface precision. A partner who handles implant cases casually is not likely to be reliable elsewhere either.
For Dental Outsourcing, implant workflow control should include early verification of implant-related information before design begins. The partner should not rely on assumption-based library matching or vague component interpretation. Instead, the team should confirm the pathway that the restoration is meant to follow and communicate clearly when essential data is missing.
This does not mean only implant-focused partners are reliable. It means implant workflows reveal how disciplined the overall system really is. A partner that handles implant cases with technical caution, clear review, and consistent logic is more likely to treat other categories with similar seriousness.
In a strange little way, implant cases are honesty machines. They reveal whether the workflow is genuinely controlled or merely looks polished from the outside.
Many teams initially evaluate a Dental Outsourcing partner by asking how fast a case can be completed. That is understandable, but incomplete. Speed matters, yet isolated fast delivery is less useful than stable turnaround behavior across many cases. A partner that returns some files quickly and others unpredictably may create more scheduling difficulty than one whose timelines are slightly more conservative but much more consistent.
A reliable partner should show realistic turnaround behavior tied to case type, case completeness, and workflow conditions. Routine cases may move quickly when the submission is clean. More complex cases may require additional review. That is normal. What matters is whether the partner handles these differences transparently and predictably.
The right benchmark is not only “How fast can they go?” but also “How stable is their process under normal pressure?” Labs and clinics need operational rhythm, not theatrical urgency. In daily dental production, dependable timing is usually more valuable than occasional bursts of apparent speed.
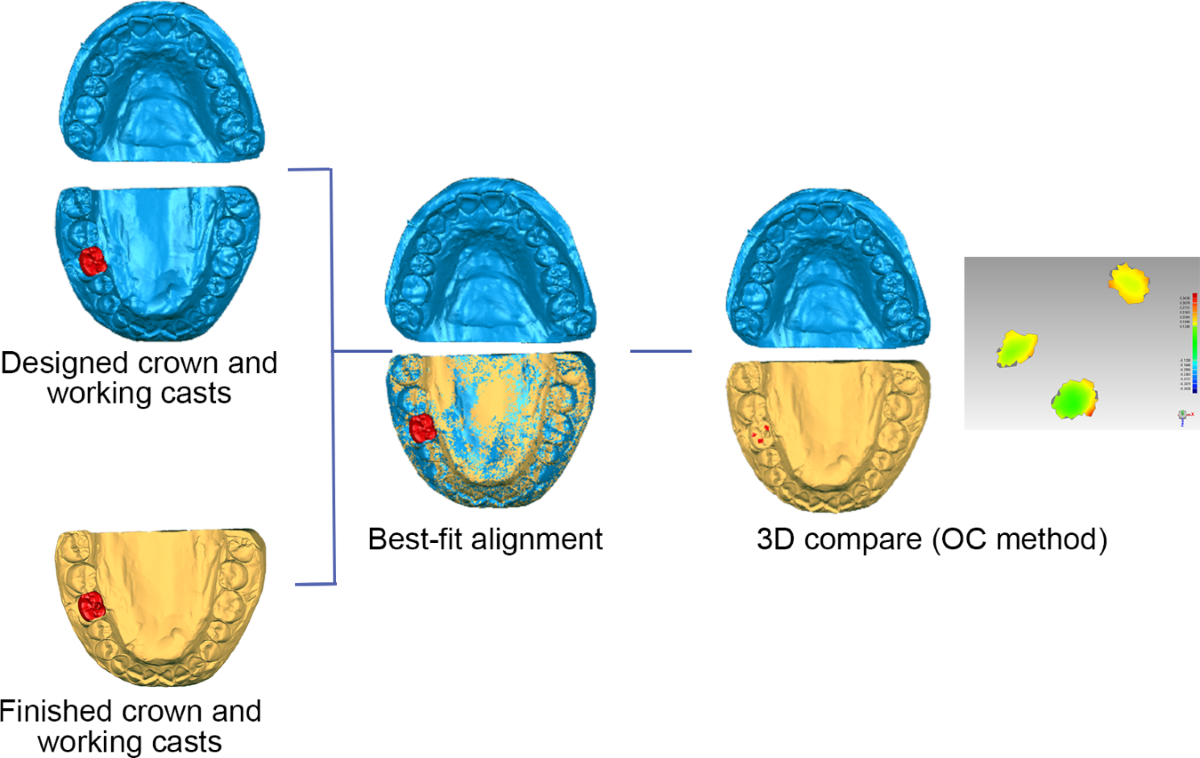
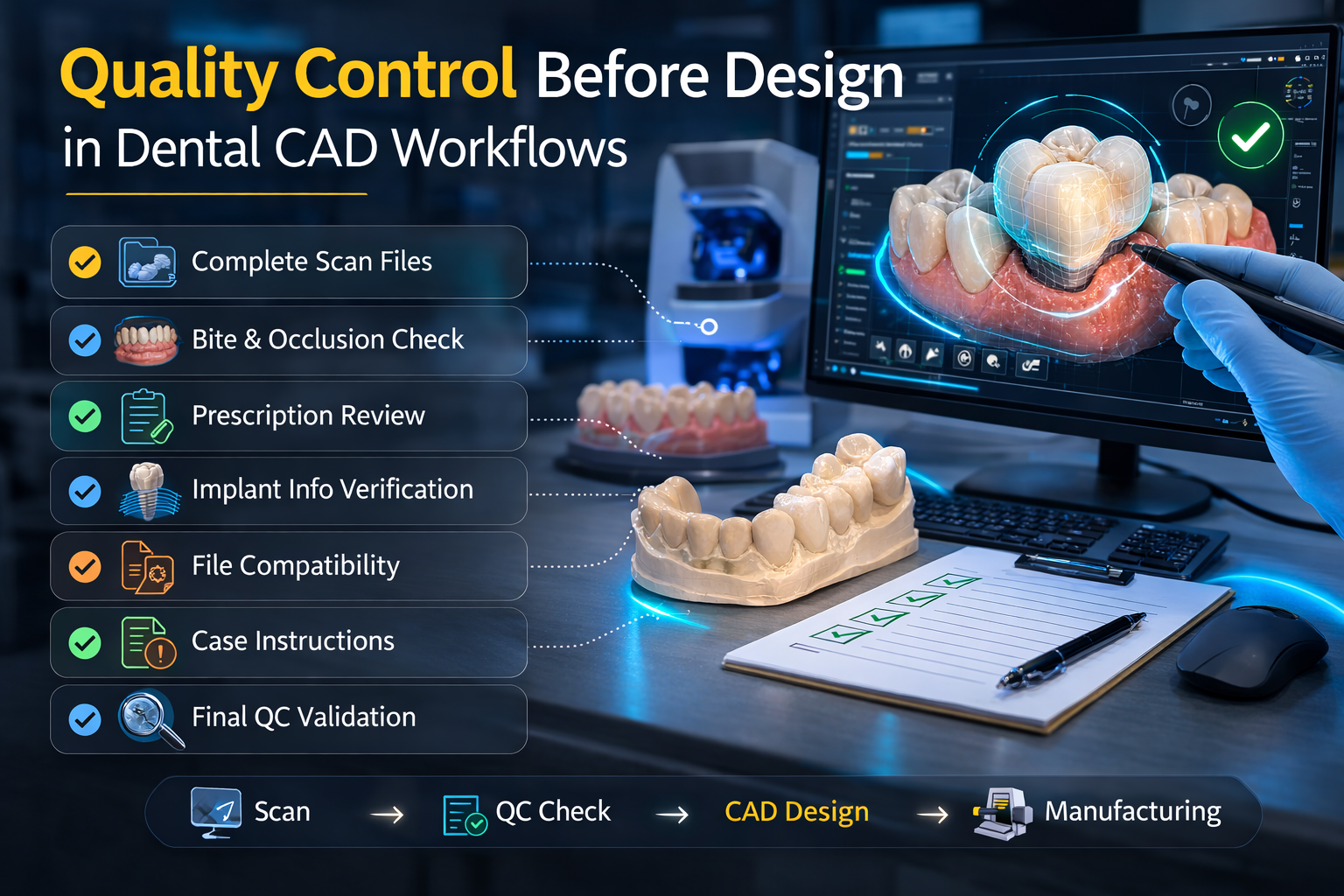
A strong Dental Outsourcing partner should not rely on one final inspection point to catch everything. Quality control works best when it appears at multiple stages: intake review, design validation, pre-manufacturing assessment, and final verification. This layered structure is one of the clearest indicators that the partner is serious about reducing avoidable errors.
At intake, QC confirms whether the case is usable. During design, QC checks fit logic, contact behavior, occlusal stability, and category-specific requirements. Before fabrication, QC helps ensure that the design matches the intended production method. After fabrication, QC confirms that the output remains aligned with the approved digital direction.
This matters because many case failures are not caused by one dramatic mistake. They develop through several smaller assumptions that pass unchecked. A layered QC model interrupts that chain earlier. For labs seeking reliability, this is far more important than generic claims about being “quality-focused.”
A partner with real quality discipline usually makes the workflow quieter. Fewer surprises. Fewer clarification loops. Fewer unstable handoffs. In technical environments, boring can be beautiful.
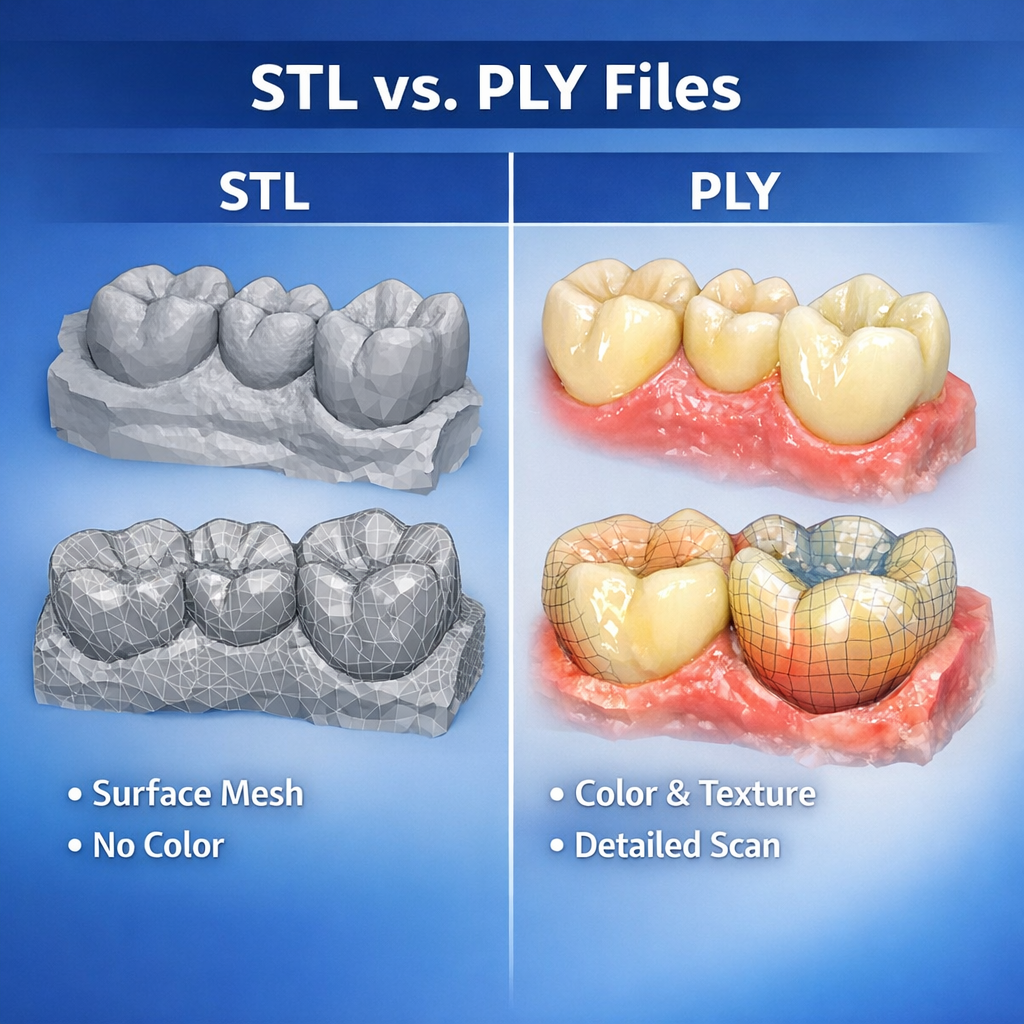
Digital workflows only remain reliable when files move cleanly between systems. That means the outsourcing partner should be comfortable handling the digital environments the submitting lab or clinic actually uses. File compatibility is not just about whether an STL or PLY can be opened. It also concerns how the full case package is interpreted, whether linked data is preserved properly, and whether the workflow avoids unnecessary manual reconstruction.
A dependable Dental Outsourcing partner should make file handling easier, not more fragile. If every submission requires repeated troubleshooting, version checks, or format reinterpretation, the workflow becomes unstable even if the technical team is skilled. The partner should have a clear process for accepted formats, linked case data, and category-specific digital requirements.
This point becomes even more important in complex restorative and implant workflows, where file completeness influences much more than geometry alone. Reliable partners do not treat compatibility as an afterthought. They treat it as part of case readiness.
One seductive trap in vendor evaluation is to focus too heavily on exceptional cases. Complex cases matter, of course, but routine case handling is often the better reliability test. A partner may perform well once under special attention and still fail to maintain consistency across daily crown and bridge volume.
For Dental Outsourcing, true trust is built when routine cases behave predictably over time. Fit logic remains stable. Contacts follow known patterns. Communication remains consistent. The team does not reinvent the wheel on every single-unit crown. This is what allows the sending lab or clinic to plan confidently and reduce the mental load of constant oversight.
In other words, a reliable outsourcing partner should not require dramatic management to produce normal results. If the workflow only works when every case is watched closely, the system is not truly dependable.
When evaluating a Dental Outsourcing partner, the most useful question is not whether the partner looks advanced. It is whether the partner reduces operational uncertainty. That includes strong intake review, clear communication, repeatable design standards, manufacturing-aware execution, disciplined implant handling, stable turnaround, layered quality control, and practical file compatibility.
These elements are not separate luxuries. Together, they define whether the outsourcing relationship strengthens the workflow or merely relocates its problems. A partner becomes reliable when the submitting team can trust the process, not just the sales description of the process.
A reliable Dental Outsourcing partner should function as a controlled technical extension of the lab or clinic workflow. The right partner does more than accept cases and return restorations. It supports predictability through disciplined intake, clear communication, consistent CAD design, manufacturing-aware thinking, implant-specific control, realistic turnaround behavior, and visible quality checkpoints throughout the process.
For dental labs, clinics, prosthodontists, and oral surgeons, this means the best outsourcing relationship is not necessarily the one with the broadest service list or the boldest speed claims. It is the one that reduces risk, supports consistency, and makes the restorative workflow easier to trust over time.
That is what reliability looks like in practice. Not noise, not bravado, not vague promises—just a workflow that behaves the way a professional laboratory partner should.
That distinction matters because outsourcing can either reduce operational pressure or quietly increase it. A partner may appear capable based on service range alone, yet still create friction through inconsistent communication, weak file handling, unclear design standards, or unstable production output. On the other hand, a well-structured outsourcing workflow can improve consistency precisely because it introduces discipline where many internal systems become overloaded or variable.
For this reason, evaluating a Dental Outsourcing partner should not begin with broad claims. It should begin with practical questions. How does the partner review incoming files? How are design decisions controlled? How does the team manage implant-specific requirements? What happens when a case is incomplete? How predictable is the workflow across routine and complex cases? These are the questions that reveal whether the partner supports reliability or merely processes volume.
Reliability begins with workflow discipline, not service breadth
A common mistake is to judge a Dental Outsourcing partner mainly by the number of services listed. A broad menu may sound impressive: crown and bridge, implants, removable dentures, night guards, surgical guides, CAD design support, and other digital solutions. But service breadth alone does not prove operational reliability. A partner can offer many categories and still perform inconsistently if the underlying workflow lacks structure.
A more useful starting point is workflow discipline. A reliable partner should show clear case intake rules, defined review steps, organized communication channels, and technical standards that remain stable from one case to the next. This does not mean every case is treated identically. It means the process is coherent enough that the submitting team knows how cases will be handled and what information is required at each stage.
From one perspective, labs want flexibility. From another, they need predictability even more. The strongest Dental Outsourcing relationships usually combine both: flexibility in case handling, but structure in process. Without that structure, flexibility turns into improvisation, and improvisation is a poor foundation for consistency.
File intake quality is one of the first signs of a serious partner
A reliable outsourcing partner does not treat every submitted case as immediately ready for production. The partner should first determine whether the file package is complete and usable. This is one of the clearest operational indicators of quality because weak intake review often leads to later delays, redesign, or remakes.
In a strong Dental Outsourcing workflow, the intake process should verify scan completeness, restoration type, bite relationships, relevant case notes, and any category-specific requirements such as implant system details or design references. If important information is missing, the partner should identify the issue early rather than designing around assumption.
This matters because a partner who begins work without validating the input may appear fast at first while actually creating hidden instability. A case that moves into CAD with incomplete data can return later with far greater disruption. By contrast, a partner who reviews before designing may appear slightly stricter at intake, but often delivers a more dependable workflow overall.
In practical terms, good intake review is a quality signal. It shows that the partner is protecting the case before value is added, not only inspecting it after risk has already entered the system.
Communication quality matters as much as technical capability
Even highly skilled production teams become unreliable when communication is vague, delayed, or inconsistent. This is especially true in Dental Outsourcing, where the external team does not share the same room, case history, or informal discussions as the sending lab or clinic. If the workflow depends on unspoken assumptions, problems tend to surface later and at higher cost.
A dependable partner should communicate clearly at three stages: before design starts, during clarification if needed, and when the case moves into completion or release. That communication should be precise rather than overly broad. The point is not to generate more messages. The point is to reduce ambiguity.
For example, if scan quality is weak, the partner should specify what is missing. If an implant case lacks component clarity, the partner should identify that directly. If a complex case needs more review time, that should be visible early rather than discovered when the expected delivery point has already passed.
There are two different kinds of outsourcing communication. One is reactive and vague, usually appearing only when something has already gone wrong. The other is structured and early, helping the case stay stable before problems grow. A reliable Dental Outsourcing partner should operate in the second mode.
Strong CAD design standards are a core part of reliability
A partner may have capable technicians and advanced software, but reliability still depends on whether design decisions are applied consistently. Similar cases should not receive dramatically different occlusal logic, contact behavior, margin handling, connector planning, or emergence design simply because they were processed on different days or by different designers.
This is why a trustworthy Dental Outsourcing partner should demonstrate stable CAD standards. Crown and bridge cases should reflect repeatable logic in fit, contact, and occlusion. Bridge cases should be designed with consistent attention to connector behavior and insertion logic. Implant restorations should follow disciplined control around component compatibility, access positioning, and restorative space.
The real issue here is not artistic variation. It is technical repeatability. Labs do not gain reliability from stylistic fluctuation. They gain it from design consistency that supports predictable manufacturing and adjustment behavior.
From one angle, CAD design is a creative technical task. From another, it is also a system task. The best partner understands both. The team must be able to adapt to case-specific demands without abandoning core design discipline.
Manufacturing awareness separates true lab partners from pure file processors
One of the most important differences between a useful partner and a weak one is manufacturing awareness. A file processor may produce a visually acceptable design. A real laboratory partner produces a design that is appropriate for how the case will actually be fabricated.
This matters because Dental Outsourcing does not end at the screen. Restorations move into milling, printing, sintering, finishing, assembly, and final inspection. If the design stage ignores manufacturing behavior, the case may look correct digitally while still performing poorly in production. Thickness management, connector structure, access positioning, internal fit logic, and post-processing feasibility all influence whether the restoration remains stable beyond the CAD phase.
A reliable partner therefore designs with production in mind. That is especially critical in implant work, long-span bridges, removable cases, and any workflow where small digital decisions can create large downstream consequences. The more complex the case, the more important this manufacturing awareness becomes.
A practical test is simple: does the partner seem to understand not just how to generate the file, but how that file will behave as a manufactured restoration? If the answer is unclear, the partnership may be technically shallow.
Implant workflow control is a major reliability checkpoint
If there is one area where reliability is easiest to expose, it is implant prosthetics. Implant cases demand stricter control because they involve more than anatomy and occlusion. They depend on library verification, scan body interpretation, retention method, restorative space, component compatibility, and interface precision. A partner who handles implant cases casually is not likely to be reliable elsewhere either.
For Dental Outsourcing, implant workflow control should include early verification of implant-related information before design begins. The partner should not rely on assumption-based library matching or vague component interpretation. Instead, the team should confirm the pathway that the restoration is meant to follow and communicate clearly when essential data is missing.
This does not mean only implant-focused partners are reliable. It means implant workflows reveal how disciplined the overall system really is. A partner that handles implant cases with technical caution, clear review, and consistent logic is more likely to treat other categories with similar seriousness.
In a strange little way, implant cases are honesty machines. They reveal whether the workflow is genuinely controlled or merely looks polished from the outside.
Turnaround reliability is more important than isolated speed
Many teams initially evaluate a Dental Outsourcing partner by asking how fast a case can be completed. That is understandable, but incomplete. Speed matters, yet isolated fast delivery is less useful than stable turnaround behavior across many cases. A partner that returns some files quickly and others unpredictably may create more scheduling difficulty than one whose timelines are slightly more conservative but much more consistent.
A reliable partner should show realistic turnaround behavior tied to case type, case completeness, and workflow conditions. Routine cases may move quickly when the submission is clean. More complex cases may require additional review. That is normal. What matters is whether the partner handles these differences transparently and predictably.
The right benchmark is not only “How fast can they go?” but also “How stable is their process under normal pressure?” Labs and clinics need operational rhythm, not theatrical urgency. In daily dental production, dependable timing is usually more valuable than occasional bursts of apparent speed.
Quality control should be visible throughout the process
A strong Dental Outsourcing partner should not rely on one final inspection point to catch everything. Quality control works best when it appears at multiple stages: intake review, design validation, pre-manufacturing assessment, and final verification. This layered structure is one of the clearest indicators that the partner is serious about reducing avoidable errors.
At intake, QC confirms whether the case is usable. During design, QC checks fit logic, contact behavior, occlusal stability, and category-specific requirements. Before fabrication, QC helps ensure that the design matches the intended production method. After fabrication, QC confirms that the output remains aligned with the approved digital direction.
This matters because many case failures are not caused by one dramatic mistake. They develop through several smaller assumptions that pass unchecked. A layered QC model interrupts that chain earlier. For labs seeking reliability, this is far more important than generic claims about being “quality-focused.”
A partner with real quality discipline usually makes the workflow quieter. Fewer surprises. Fewer clarification loops. Fewer unstable handoffs. In technical environments, boring can be beautiful.
Case compatibility and software handling should reduce friction, not create it
Digital workflows only remain reliable when files move cleanly between systems. That means the outsourcing partner should be comfortable handling the digital environments the submitting lab or clinic actually uses. File compatibility is not just about whether an STL or PLY can be opened. It also concerns how the full case package is interpreted, whether linked data is preserved properly, and whether the workflow avoids unnecessary manual reconstruction.
A dependable Dental Outsourcing partner should make file handling easier, not more fragile. If every submission requires repeated troubleshooting, version checks, or format reinterpretation, the workflow becomes unstable even if the technical team is skilled. The partner should have a clear process for accepted formats, linked case data, and category-specific digital requirements.
This point becomes even more important in complex restorative and implant workflows, where file completeness influences much more than geometry alone. Reliable partners do not treat compatibility as an afterthought. They treat it as part of case readiness.
Consistency across routine cases is often the best proof of trustworthiness
One seductive trap in vendor evaluation is to focus too heavily on exceptional cases. Complex cases matter, of course, but routine case handling is often the better reliability test. A partner may perform well once under special attention and still fail to maintain consistency across daily crown and bridge volume.
For Dental Outsourcing, true trust is built when routine cases behave predictably over time. Fit logic remains stable. Contacts follow known patterns. Communication remains consistent. The team does not reinvent the wheel on every single-unit crown. This is what allows the sending lab or clinic to plan confidently and reduce the mental load of constant oversight.
In other words, a reliable outsourcing partner should not require dramatic management to produce normal results. If the workflow only works when every case is watched closely, the system is not truly dependable.
What a lab should really be looking for
When evaluating a Dental Outsourcing partner, the most useful question is not whether the partner looks advanced. It is whether the partner reduces operational uncertainty. That includes strong intake review, clear communication, repeatable design standards, manufacturing-aware execution, disciplined implant handling, stable turnaround, layered quality control, and practical file compatibility.
These elements are not separate luxuries. Together, they define whether the outsourcing relationship strengthens the workflow or merely relocates its problems. A partner becomes reliable when the submitting team can trust the process, not just the sales description of the process.
Conclusion
A reliable Dental Outsourcing partner should function as a controlled technical extension of the lab or clinic workflow. The right partner does more than accept cases and return restorations. It supports predictability through disciplined intake, clear communication, consistent CAD design, manufacturing-aware thinking, implant-specific control, realistic turnaround behavior, and visible quality checkpoints throughout the process.
For dental labs, clinics, prosthodontists, and oral surgeons, this means the best outsourcing relationship is not necessarily the one with the broadest service list or the boldest speed claims. It is the one that reduces risk, supports consistency, and makes the restorative workflow easier to trust over time.
That is what reliability looks like in practice. Not noise, not bravado, not vague promises—just a workflow that behaves the way a professional laboratory partner should.